From the Wall Street Journal:
And from earlier this year in Idaho:
The 2012 merger of two health care providers in Idaho’s second-largest city, Nampa, was properly found to violate Section 7 of the Clayton Act, the U.S. Court of Appeals in San Francisco ruled today. A decision of the federal district court in Boise, ordering St. Luke’s Health System, Ltd.—the largest health care system in Idaho—to divest Saltzer Medical Group—the state’s largest independent, multi-specialty physician practice—was upheld
These are the next frontier of healthcare reform. We, as a nation, are committed to treating most healthcare in a quasi-market like manner. To do that so that we have effective and cost effecient care means actually treating the two major sides of the healthcare market (payers and providers) as markets that deserve significant competitive scrutiny. An activist Department of Justice and a Federal Trade Commission that has a default assumption that consolidation among major actors is anti-competitive unless clearly shown otherwise is a good thing.
Let’s remember what the basic market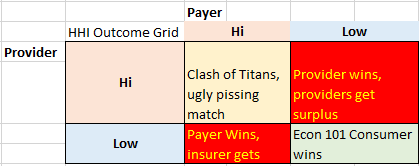 structure of payers and providers looks like in the United States.
structure of payers and providers looks like in the United States.
Dominant insurers use their ability to steer hundreds of thousands patients to or from different providers as a stick to get rates that are based on Medicare with a small kicker. This works because a dominant insurer does not need to get every provider in a specialty or concentration into the network. They just need to get enough providers in network to satisfy state regulators. Providers who don’t take the low rates from the dominant insurer have a hard time making up at higher price points the revenue they lose in volume. Areas where there is a single dominant provider in either the entire market or a critical set of specialties will see the providers tell insurers “You either take my rate, or you can’t sell in this county as I’m the only provider in the region…….
Areas where there are a multitude of medium and small payers who can’t threaten the economic existence of a multitude of fragmented providers see effective competitive bidding. Providers can not name their price as insurers and other payers can walk across the street to another provider and sign a deal. Insurers can’t force prices down too much as each individual provider has half a dozen other options to make a living. And finally, areas where there is a single dominant provider and a single, dominant payer see very nasty fights over rents.
The worst case scenarios is the Provider highly concentrated with the payers fragmented as reimbursement rates are high and utilization is probably high. Concentrated payers with fragmented providers will see low reimbursement rates, and the potential for low premium rates as benevelent local non-profit insurers might keep rates low. Otherwise, the executives get lots of high quality blow and flexible hookers as the insurance company is bloated and inefficient. The ACA’s requirement on minimal Medical Loss Ratio of either 80% (individual and small group) or 85% (large group) has crimped the blow supply.
Situations where both the payers are highly concentrated and the providers are highly concentrated are probably the second best outcome. As long as there is no evidence of collusion, big payers fighting big providers keeps pricing reasonable although quite a bit of market surplus is consumed as both sides piss at each other.
Finally, the best case scenario is fragmented markets where there are efficient payers and efficient providers who are effectively price takers and not price makers. Here consumers get good prices on good care.
There are not too many regional health markets that can be categorized as Econ 101 utopias where everyone is a price taker. I don’t think the DOJ or FTC can create those types of markets even if they had the legal authority to do so. However, a suspcicious DOJ and reluctant FTC can aid in preventing Low-Low situations from going to High-Low or Low-High rent extraction situations. And more often prevent a Medium-Medium situation from going to a Medium-High situation.
Baud
The plan is to let them all consolidate into one provider and then single payer, bitches. #CheckandMate.
Richard mayhew
@Baud: okay when does that happen?
Richard mayhew
@Richard mayhew: actually we would want single payer and lots of providers to really get low pricing
Baud
@Richard mayhew:
May 23, 2027.
MomSense
@Baud:
ha! Future President s/he sold us out!
japa21
Lots of rumors flying as to possible mergers and/or buyouts. One of the biggest is the rumor that Anthem is looking to buy CIGNA. I really have difficulty believing that would get past the DOJ.
japa21
@japa21: Should point out that I work for neither of them.
ThresherK
That a somewhat non-ignorant from two timezones away (like myself) couldn’t name “Nampa” as the second-largest city in Idaho, a big and sparsely populated state, should indicate how badly the competition is needed there.
Let it all merge, and these folks won’t have a choice for hours and hours around, even if they have the money and time off from work to drive it.
Punchy
Can we get a SCOTUS open thread, now that EPA and redistricting is about to be announced?
kaythanxbouy
JPL
@Punchy: We know they are hearing affirmative action again next term. So much for the court moving left.
Roger Moore
@Richard mayhew:
No. We want one payer/provider, i.e. NHS.
Gene108
About 15 years ago there, iirc, there was a lot of consolidation in insurance carriers, which coincided with the rapid spike in health care costs in aughts.
Not sure if this is a cause, but it is an interesting thing which I hope is being studied.
mb
@Richard Mayhew: I’d be interested in a post from you focusing on the implementation of the employer mandate. Seems to me the timing of it coinciding with the election year is unfortunate. Regardless of the reality, the Rs are going to play up any angst it causes. I guess my question for you is: is the employer mandate implementation going to be traumatic?
Richard Mayhew
@mb: Short answer — not really as most employers of more than 50 people already offer minimally qualified plans (Bronze or better), and vast majority offer Silver or better plans.
Low wage, low margin businesses like Darden, Papa John’s will bitch and moan, but they’ll comply as total exposure is fairly low as the numnber of non-managers who get more than 30 hours per week is not a high % of work force.
Lots of sound and fury signifying Meh
Arclite
@Baud: Heh, came here to post the same thing. Let ’em merge then nationalize the whole thing into single payer. =D
Arclite
@Richard mayhew: Ah, yeah, true.
Arclite
@ThresherK: In Japanese, “nampa” means picking up a girl off the street and having sex with her.
mclaren
Once again, Richard Mayhew his lying to you. His subtext, beaten like a drum, is that things are getting better every day in every way because of the ACA.
Meanwhile, drug prices skyrocketed by 13% last year.
The TPP, which Obama traitorously fast-tracked with the help of his corporate crony Democrats, will send health care costs through the roof:
Source: “Why TPP sucks,” Crooked Timber website, 12 June 2015.