The Rand Corporation recently looked at actual claims data for employer sponsored coverage in the state of Indiana. They were primarily looking at hospital costs. The short finding is that there was massive variation in charges with some hospitals charging just a bit more than Medicare rates and other hospitals being paid three, four or five times Medicare rates.
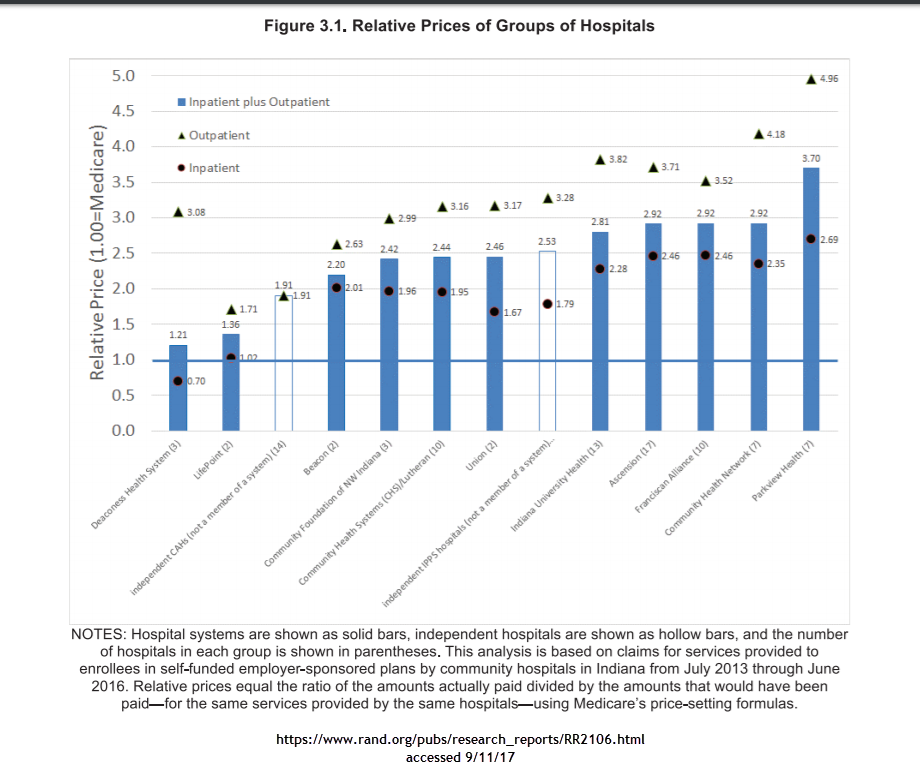
There are a lot of policy points that can be taken from this graph. The first is that there may be a strong public interest in breaking up some of the larger chains. The second will be the perennial cry of all payer rate setting so standardized rates are offered. The third is that there is an oddness in that outpatient services which are theoretically more easily competable and shoppable are much more expensive relatively speaking than in-patient services.
Indiana’s pricing configuration invites narrow and tiered networks. Narrow networks are a way for an insurer to say no in order to get good pricing. Looking at the graph, a narrow preferred tier of Deaconness, Lifepoints and the independent critical access hospitals with a non-preferred tier of everything before Indiana University hospitals with a carve-out deal to send high end complex cases to one of the tertiary care hospitals makes a lot of economic sense. That type of network design offers a decent number of hospitals while trying to send people to the least expensive places of care. It also involves saying no a lot in order to get a better premium. That act of saying no disrupts current relationships and that produces screams.
But in the short term, if one wants lower premiums, that means expensive providers have to be minimized. Narrow networks with tiering and steering is the tool that accomplishes that goal.
Tom
While I’m a big fan of lowered health care costs, how much does the cost of living differential (e.g., San Francisco versus Bloomington, Indiana) factor into the differential pricing?
David Anderson
@Tom: Indiana is historically a high price state for medical and hospital care even though the cost of living is fairly typical for the US.
Major Major Major Major
@Tom: @David Anderson: do Medicare or Medicaid rates differ by region?
Villago Delenda Est
Hmmm….ok, so this strategy works short term. How about long term?
Also, disrupting relationships and producing screams might make sense strictly from an economic point of view, but what if the relationship in question is between doctor and patient?
Mel
@Villago Delenda Est: This, absolutely!! Not all doctors are the same, by a long shot, and not all doctors are good at treating all types of patients.
If your life or that of a loved one is on the line, do you want to be forced to go to the specialist who blares Rush Limbaugh on his office tvs, never returns calls, and changes his demeanor when he realizes that the patient in question has a disability? Do you really want to find out that you have to go 50 miles further each way, to a hospital with a significantly higher infection rate and a much higher rate of malpractice suits because, Yeah!, narrow networks mean more profit for CEOs and stockholders, while causing a small upfront premium deduction for policy holders. Believe me, the first time anything serious happens to someone you love, orsoneone requires more than cursory care for common, in-office treatable illness, that narrow network becomes not such a good idea.
sharl
OT – Betty Cracker has checked in:
Mel
@sharl: Sharl, thanks for the update! So glad that Betty and Co. are okay! Hoping everyone else is safe as well!
japa21
I know Indiana well, as it was one of the states I was responsible for when I was doing network contracting. IU and Franciscan were (and probably still are) notorious not only for demanding high reimbursement, but also some level of exclusivity in the areas they represented outside of the Indianapolis metro area. Only Minnesota was worse, and that is because they pretty much required a percent off billed charges reimbursement.
IU was also busy expanding its ownership of hospitals throughout the state, although they did not have the same demands for all the facilities. My guess would be if they separated the Indy area facilities from the rest of the hospitals, there would be even a more stark difference.
Capri
My employer tried to steer patients to lower-cost options via an on-line tool that was part of the available health benefits. You plugged in what procedure you need, and it directed you to the lowest priced provider in your area. It was dropped after 2 years because it was hardly ever used. The biggest reason was that patients trusted their physicians and basically did what they said. Secondly, it’s very easy to explain how going with lower cost options helps the insurance companies, but as the system is currently structured, it has little impact on the patients.
efgoldman
Wouldn’t you expect this in a medium-sized state which has both major teaching hospitals and rural hospitals?
David Anderson
@efgoldman: pretty much yes… @Capri: Lower premiums = higher take home pay especially if the offer at work is structured as narrow network at minimal or no employee contributions with the broad network at a significantly higher rate for the employee.
jl
” The second will be the perennial cry of all payer rate setting so standardized rates are offered. ”
Many countries have mechanisms that try to get as close to this as possible. So, it is a perennial cry that is never answered in the US but not other countries.
Regional industry negotiations for uniform charge (called tariffs in other countries), or a band of acceptable charges is one way to get close to that goal. For it to work there has to be a representative of the payer groups, and, as far as possible, neutral arbiter with audit power.
I’m not sure what role legal and regulatory frameworks versus interest group political and financial power play in preventing this approach in US.
Edit: this has been another comment in my ‘Go Swiss’ series. Or Netherlands.
Eric
@Capri: In general I think that most doctors would have a hard time even attempting to refer patients to a lower-cost provider/resource. Its interesting that your employer could build such a tool but I don’t believe many physicians have a similar tool that they can use for referrals. Instead, they’ll refer to who they know, trust, and have heard good things about.
Eric
@japa21: Sorry if this is common knowledge but what does “required a percent off billed charges reimbursement” mean? This isn’t really my area but I’m interested in learning more about how insurance, marketplaces, etc. work.