The White House budget is out. It is dead on arrival. However it is still a useful document as values drive money and money reveals values. There is one quick segment I want to highlight.
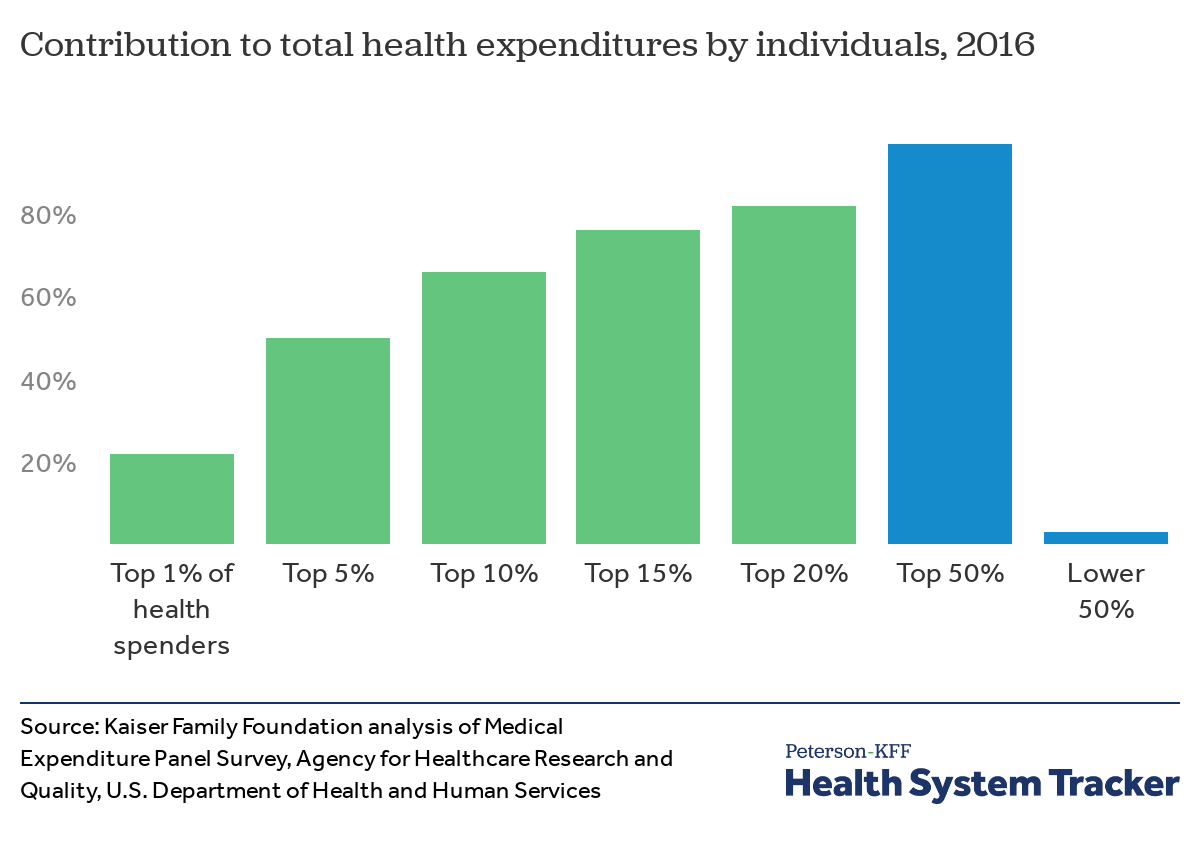
10% of a lot of dollars is still a lot of dollars, especially in a TV ad in a competitive district. It is grossly insufficient. Costs in the US healthcare system are tremendously skewed. Most of the population barely touches the healthcare system. They might have a vaccination and an urgent care visit or they may not even go to the doctor during the year. Anything works well enough for this cohort once it is retrospectively identified.
But the real costs of the system are concentrated in very few people.
The Peterson-Kaiser Health System Tracker has updated the cost share of various percentiles of spending in the US Healthcare system. They show very little new, but confirm that most costs are concentrated in few people.
10% of a much smaller block grant that is designed to shrink in real GDP terms over time is a trifling insult. It places incredible risk and costs on the sickest part of the population.
This is a value statement.
catclub
how would that chart change if you put it in terms of ‘last six months of life’?
My suspicion is that lots of people in that last column – lower 50% that only have 3% of costs,- suddenly get into the top spending category.
eventually everybody gets to last six months of life. It is not like everybody is temporarily financially embarassed millionaire.
alternatively the expensive group IS those who have expensive, complicated diseases for a long time.
Mary G
As someone who’s had rheumatoid arthritis since the late 70s that’s been treatment-resistent, the message has been heard loud and clear from Republicans: die already, you cost too much.
dr. bloor
They’re all in on the “Die Fast” model of care. It’s only a matter of time before someone floats a Carousel Model of late life care a la Logan’s Run.
debbie
@catclub:
I’m not sure you’re right. I think the expensive group is the long-term chronic group. They’re the people who live on despite their conditions.
debbie
@Mary G:
I’m in a similar boat, since 1987. I expect I’ll return to uninsured status when I leave my current job.
chopper
@Mary G:
ah yes, the “single prayer” health care system.
ProfDamatu
@debbie: I’m not positive, but I think it’s a little of column A, a little of column B. I don’t have the figures at hand, but if you look at the medical spending amounts that put you into the various percentiles, you find that some of the folks in that most expensive category are indeed people in the last 6 months of their lives, who die from something that instigates a lot of intervention (and of course just nursing or hospice care isn’t cheap!). Others will be people with long-term, chronic illnesses. But there will also be people who are in and out of that high-cost group. Some of them might be literally “hit by a bus;” surgery and rehab from serious accidents will do it. Then there are the metaphorical “hit by a bus” people like me. I haven’t run the numbers, but I would guess that in the two years that I underwent cancer treatment (late 2013-early 2014 for lymphoma, 2016 for breast cancer) I was most likely in the top 5%, if not the top 1% of health spend; between and since, I’d guess I’m pretty close to being in the bottom 50%.
Ohio Mom
Hey, what’s this about “beginning 2021…the Medicaid BLOCK GRANT (emphasis added)”?!
Medicaid is not a block grant, are they trying to sneak that in?
If so, you can expect another round of angry people in wheelchairs protesting.
Medicaid is what allows disabled people to live in their communities. It provides the supports (such as personal aides, equipment, transportation, job coaching, leisure activities, etc.) necessarily for meaningful lives.
Sign me,
A mom approaching her dotage who lives for the day her son receives enough Medicaid funding to live in a supervised living situation so she can rest easy, knowing he’ll always be taken care of. Which won’t happen if Medicaid is cut, which is what block-granting would be.
rikyrah
@Ohio Mom:
They know that it’s dead until then.
November 2018 has protected the American Social Safety Net. That was one of the byproducts of the election.
So, see you November 2020, muthaphuckas. Good luck on running on this.
debbie
@ProfDamatu:
You’re far better at running numbers than I will ever be! I think the number of people with chronic life-long conditions far outweigh acute or end-of-life issues.
I’ve got a doctor’s appointment in a couple of hours and I’m going to ask her about this.
sherparick
As flawed human being Alan Grayson said, the Republican Plan is “Don’t get sick, but if you do, die quickly.”
Ohio Mom
@debbie: Also, I suspect a lot of people with chronic conditions have more than one, so that could muddy the count. Say, if you count people with Type 2 diabetes and people with high blood pressure separately, that would give you a higher number than the number of actual patients.
This is why I was an art major. My eyes are glazing over already.
@rikyrah: I’ll try repeating that to myself in between deep breaths.
Still, the special needs parents in my red suburb will continue to vote for those, as you so elegantly put it, muthaphukers.
debbie
@Ohio Mom:
Say no more. I too was an art major.
gene108
@debbie:
Some chronic conditions, which respond to standard treatments aren’t going to break the bank, with regards to expenses.
The costs are already set, so insurers know what the costs will be.
A lot of the issue is not usage, but on what providers charge. In the end all the bloated spending we have on healthcare goes to the providers. They have to take a reduction in pay (for lack of a better term), in order to reduce costs.
Unfortunately, a lot of us like our doctors, and if doctors en masse protest a cut in pay, a lot of folks will side with their doctors, rather than ways to curtail healthcare spending.
debbie
@gene108:
Chronic conditions are managed, not cured. The costs don’t go away.
Mike in NC
House Democrats should propose a budget that sets aside exactly $1.00 towards funding Fat Bastard’s precious wall.
Bnad
Are there stats on how many people find themselves in that annual top 5% or top 1% at some point in their life?
JaySinWA
Republican health care has no death panels, just ‘unbiased’ financial constraints that kill people.
Gin & Tonic
Didn’t candidate Trump run on “I will never cut SS or Medicare”? It seems like so long ago, I can’t recall.
azlib
This chart also explains why the conservative idea of funding high risk or high cost consumers in a separate insurance pool is a sham. There is no way such a pool is ever adequately funded from general revenues given the skewed distribution.
catclub
@Bnad:
That was why I asked about measures during the last 6 months of life.
Uncle Cosmo
Does anyone really think that (e.g.) a month’s supply of insulin costs anywhere north of $100 to produce?
Is it any wonder that no one seems to be making any progress on figuring out the ultimate cause of insulin resistance (i.e., type II diabetes), let alone finding a cure?
IMHO the entire health-care/assisted-living sector is little more than a scam to suck any wealth the lower & middle classes might have accumulated back into the pockets of the plutocrats.
Yutsano
*waves from that 1% high usage column*
I’m definitely in the high utilizer category for various reasons. I’m rather expensive to keep healthy. I just happen to be lucky enough to be able to have good insurances to cover me. It’s interesting that even Canadian health care could be expensive for me because I take several expensive medications. As RedKitteh once told me, medical bankruptcies in Canada are rare, but they do still happen, mostly related to drug costs. So even single payer is not necessarily a panacea.
Brachiator
@ProfDamatu:
I’ve seen studies that suggests that this is exaggerated. I am sorry that I don’t have the links at hand just now. Hopefully others will be able to chime in.
rikyrah
@Uncle Cosmo:
Does anyone really think that (e.g.) a month’s supply of insulin costs anywhere north of $100 to produce?
Absolutely not, which is why I think they are colluding on the price.
David Anderson
@Brachiator: The big problem for the end of life cost question is how do you know prospectively when someone is going to be dead in six months?
Retrospectively, that is really easy, but prospectively, that is one hell of a nasty problem that gets into ethical quandaries really quickly if it was to ever be acted on.
Ohio Mom
@Uncle Cosmo: And just in case some troll wants to pipe in that Walmart sells a vial of insulin for $25, there are all sorts of insulin that are designed to work over different time spans, such as short-acting and long-acting.
The longer acting stuff makes a big difference in keeping blood sugar levels even over time and guess what, Walmart isn’t selling the newer, better types of insulin.
Walmart sells the type that forces you to eat on a very strict schedule, time-wise and carb-wise. Yes, it’s better than no insulin at all but it is very sub-optimum. Few people can focus their every moment, waking and not, on monitoring and maintaining an appropriate blood sugar level. They usually have other activities that need attending to (work, children, chores, etc.)
ProfDamatu
@Brachiator: Possibly; I recall reading that last 6 months was a huge fraction of Medicare spending, but that doesn’t necessarily mean that it’s a huge fraction of *all* spending. In any event, I wasn’t suggesting that it was the main factor – *some*, but not all, in addition to expensive chronic conditions and one-off big-ticket years from otherwise healthy people. :-)
I tend to feel that although it’s probably useful to look at expenditures over those last 6 months, the utility is probably more in terms of finding out how much care that ultimately does no good (very broadly defined) is happening. I’m more skeptical of its value in bending the cost curve significantly, if only because the last 6 months of a person’s life can only be determined in retrospect. If we found out that say 50% of all spending was indeed in those last 6 months, I’m not sure how that directly translates into policy aimed at reducing costs.
All I know for sure is that it’s very complicated!
ProfDamatu
@David Anderson: Lol, and this is why I shouldn’t start writing a comment during a break in class and finish it afterward!
I agree, that last 6 months metric really has the potential to get ethically problematic super fast. I’d hate to think that insurance companies would start throwing up roadblocks on that basis, but I’m cynical enough to suspect that at least some of them absolutely would.
ET
Would high cost individuals count that boy whose parents got him no vaccinations/shots and he got lock-jaw and nearly died? He care almost cost $1 million and the article I read said his parents don’t plan on getting him any.
Brachiator
@ProfDamatu:
Yes. This is the key issue in some of the stuff on this I had been reading. You can’t predict end of life accurately, so a lot of situations end up being lumped together.
Also, one cross-country study came to the following conclusion:
One side issue I find interesting is that medical costs may be increasing simply because there are more people age 65 and older than in earlier years (in absolute numbers, not just as percentage of a country’s population). In some ways, this should be expected as overall quality of life improves in industrialized countries. But it also means that you may have to make adjustments.