Last night Ruemara made the very good point that the prices that we pay for healthcare are ridiculous and that the split between insurance types that really comes into play above the shoulder blades is nuts.
The solution, it turns out, is cutting open my gum & stuffing it with, uh, bone, I believe. Like stuffing a bra with tissues only the hope is the tissues will bond with the boobies to build healthy bone in the jaw. Or something like that. This procedure costs $3k. With insurance. Which is a yikes. And a “motherfuck, is this going to give me superpowers, at least? ” Because, yikes, and on both sides of my jaw. Double yikes.
There is one point I want to circle back to though:
making healthcare affordable will require addressing the scale of costs in the U.S. for medicine, tools, personnel, materials — the whole shebang. I don’t believe Medicare for All addresses that except with the idea that we excise insurance companies from the equation.
The logic model of this statement is that the traditional Medicare program spends about 5% of total program expenses on administration and overhead while the ACA allows insurers to spend between 80% (individual and small group) and 85% (large group) of premiums on claims and therefore spend between 15% and 20% on administrative overhead, hookers and blow for the C-suite and profit. Squeezing 10 points from the hookers and blow accounts and profit would lead to lower prices.
To a limited extent, that is probably right. But it is a very limited extent.
There are two things we must consider though. First the denominator problem. [Total Claims/ (Total Claims+ Admin Costs ) ]*100 is how we get the 95% figure for Medicare. We don’t know if we are at an optimal level of administration for Medicare. The easiest way to make the number go up is to increase total claims as that increases the numerator faster than the denominator. This metric rewards spending a lot on ineffective claims and very little on non-billable services that are far more effective and efficient. As a subpoint, efficient insurers can be profitable at 88% to 90% MLR and at least some of the money that they spend between 88% and 95% is on administrators that adds system complexity in forms such as bundled payments, care coordination and alternative payment models that lowers total cost of care that accrues directly to the payer and also has positive,cost reducing system delivery spillover savings. We want care delivery changes that leads to lower total spending and sometimes that involves substituting clinical claims dollars for administration dollars.
Secondly, insurers aren’t where the money is. I am pulling up Table 3 of the 2017 National Health Expenditure.
The graph has source of spending for everything except 3rd party and other sources of funding as this is quick and dirty.
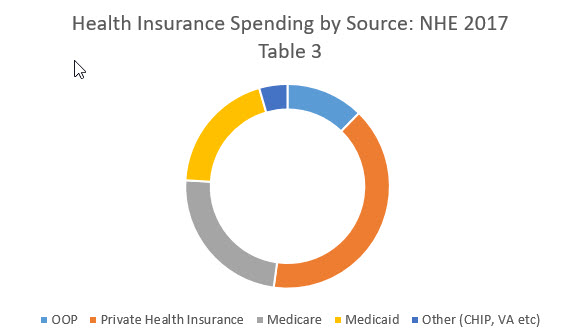
Private health insurance makes up about 40% of the spending in this subset. 12% is out of pocket spending through either direct cash payments or cost sharing which comes from either private insurance, Medicare or other types of insurance. The rest is government spending. Eliminating 10% of the spending from the administration of private insurance leads to a one time 4 point drop in national health expenditures in a static analysis. I think the actual drop in this scenario would be significantly less as I think that at least some of the work that my former co-workers do every day is not pointless red queen racing or performative preening.
Making insurers more efficienct is a good thing. I am not disputing that. However moving every insurer to a theoretical optimal level of administrative leanness (I am not assuming it is the Medicare level) that is higher than the current average level of administrative efficiency will only produce a couple of points in change for a single year. The real money is not at the insurers. And that insight is why Colorado is trying to institute price banding on hospitals in their public option plan.
gene108
Thank you for making this clear.
Betty Cracker
I’m guessing you didn’t work in the marketing department. Earlier in my career, I did work for an insurance company marketing shop. In addition to writing brochures and ad copy, one of my jobs was composing letters to members designed to maximize the scare factor so they’d decline to access services the insurance company was required to cover. “Needle biopsy” instead of plain old “biopsy” when discussing procedures involving an insured person’s scrotum, that sort of thing.
No doubt thousands of former English majors were drawing salaries in thousands of similar positions, just random cogs in the wheel of a thoroughly evil machine. Don’t even get me started on the fucking lobbyists…
FlyingToaster
Private insurers — or at least those provided through employers — are already banding the providers.
Our BCBS HMO plan calls itself “Hospital Choice” and puts a surcharge if you go to one of the main Partners hospitals, or some of the Longwood specialty joints. Our hospital is also a Harvard teaching hospital, but it’s not in Partners, so it’s cheaper.
Partners: Mass General, Brigham & Womens. Longwood: T stop surrounded by hospitals, including Boston Children’s and Dana Farber Cancer Institute.
satby
This may be a question you can only guess at, but how much of the medical cost in this country is because of practice limitations (only medical drs. can perform x, only procedures done by y are reimbursable)? And how much is because of overtesting as a liability protection?
it seems like even if they were smallish percentages, adding that to the cost savings you detail above starts to add up to a decent reduction in overall cost.
low-tech cyclist
I’ve never understood the reluctance of health care reformers to go after hospitals.
I don’t know when we went from hospitals with names that were variations on [County Name] Hospital and [Denomination] Hospital and the like, to corporate-owned hospital mega-chains* – that’s a story I’d like to hear sometime – but they’re just another corporate profit center now, and have been for decades.
Not to mention the whole surprise billing bit when you have a procedure done at an in-network hospital, but that doesn’t mean shit because if the doctors aren’t also in network, you can be hit with thousands of dollars in unexpected charges.
I can understand people thinking, “I like my doctor, don’t cut costs at her expense,” but do they really feel that way about their hospitals too? I have a hard time believing that.
* For instance, I’m old enough to remember when Inova Fairfax Hospital, near where I grew up, was Fairfax County Hospital.
Butch
At the same time….I was charged $244 for a pneumonia shot plus a $53 fee for administering the shot. I think there are plenty of places to find more efficiency.
Chyron HR
@low-tech cyclist:
Bernie didn’t tell them to hate hospitals, so they don’t care. QED.
Bill Hicks
There seems to be a problem with the formula listed above. Total Cost/Total Cost + Admin is the same as 1+Admin. I think you meant Total Cost/(Total Cost + Admin) with x100 needed for percent.
DAVID ANDERSON
@Bill Hicks: yes I forgot my brackets
wvng
David, thanks for this. I get in discussions about this all the time. Insurance has to pay for care, and it is the cost of care that drives the price of insurance. Making changes to insurance providers only changes insurance costs at the margins.
Capri
For anyone interested in this topic I’d recommend the book The Price We Pay by Marty Makary. He’s a John Hopkin’s surgeon who has been researching the cost of medicine for years. He does a very good job explaining how we got this way and suggesting ways to improve. A huge driver of cost is good old fashioned price gouging on the part of the hospitals and doctors. But all the legacy players bear some share of the blame.
David Anderson
@Betty Cracker: Note I limited and qualified my statement;
I can think of several floors of former co-workers (including most of marketing) that were engaged in red queen racing or compliance or nest padding… I can think of at least one and a half floors where that is not the case.
lashon harumph
@David Anderson: I would greatly appreciate if you could spend more time explaining the cost structure of US health care. One reason universal coverage is hard to do is our costs are so much higher than any other developed country. Even if we had M4A, the current cost structure means we will have less tax revenue for all the other things we need to fix. This issue may not be your core area of expertise but perhaps you know folks who could guest post.
Another Scott
Economists like to make the point that there’s a huge difference between levels and rates-of-change. That’s why almost nobody reports the actual GDP of the economy any more – what matters is how quickly it is changing.
Isn’t that the real issue with healthcare costs as well? We’re sorta muddling through (on the whole, but not in details) on paying the total cost, but the rate of change is not sustainable. Healthcare+insurance is too big a slice of the economy now to continue to have annual increases far in excess of the overall rate of increase in the economy. It’s not sustainable.
What’s driving the continuing large price increases? The cost curve bent slightly during the Great Recession and when Obamacare kicked in, but isn’t it still something like 3x the CPI?
We know that physicians aren’t going to accept a sudden 50% cut in incomes. Hospitals and Medical Supply corporations and Pharmaceutical giants aren’t either. The only way to get there is through cutting the rate of increase in costs while catching abuses, instituting more rational policies, etc.
We hear the horror stories of Medicare fraud in FL and opiate/opoid fraud in WV and all the rest. It’s a huge amount of money, but it seems like small potatoes overall.
My solitary GP felt he had to combine with a larger medical practice when Obamacare kicked in (apparently because of the new rules and paperwork). Is centralization and lack of stand-alone medical groups driving up costs the way hospital consolidation is? I haven’t noticed a change in my costs, but there is a lot more computer stuff in his practice now…
(Insert other personal anecdotes about expensive, wasteful throwing out of perfectly good drugs and medical supplies, hospitalization, etc., etc.)
And isn’t it true that the US-pays-twice-as-much-as-other-advanced-economies gap closing over time? Aren’t costs rising in the rest of the world as well? (Yes, we still pay a lot more than other countries – for poorer outcomes – but the savings may ultimately be smaller than we think.)
As you point out, there are lots and lots of players and they’re all going to yell and scream to keep their incomes and their slices of the pie. We need to think carefully about where the money is going, where the annual increases are coming from, and what we do about it.
Thanks. You continue to provide a great service with these posts.
Cheers,
Scott.
Betty Cracker
Another book rec: “An American Sickness: How Healthcare Became Big Business and How You Can Take It Back,” by Elisabeth Rosenthal, also an MD.
germy
Matt
The mean doctor income is $300,000, at least six times the average income.
Downpuppy
In addition to insurance co administration, the medical side expense of dealing with the insurers – getting them to actually pay – is pretty significant.
Barbara
We pay more on a per unit basis for every kind of medical service than anywhere else in the Western world, and that is regardless whether the country has adopted a national health service (England) or an insurance scheme (Netherlands, Switzerland) or something in between like France or Germany. We. Pay. More.
We also expect more, and really, we expect more than it is reasonable to assume that medical care can provide in the way of returns if the measure is improved health outcomes. This is a position that has been embraced by health care providers as well, but mostly, we would see better return for our dollars by investing in green space, outlawing guns, giving people more money and nutritional counseling and so on. I am not holding my breath for these things to happen but it’s important to bring a realistic eye to what we should be expecting from and paying for health care intervention. Right now, it almost feels like we are all players at a slot machine, who just know that if we keep putting money in we will get the big pay out. Nope.
@Betty Cracker: “Earlier in your career” presumably means prior to the institution of MLRs as a matter of law. Yes, insurers pay to market themselves, but seeing this through the lens of different kinds of insurers, the more successful ones are much more efficient in the way they market.
What Have the Romans Ever Done for Us?
I keep coming back to price gouging. One way to stop it is to require providers to give people seeking service some idea of the price that will be charged. I recall hearing an NPR segment on outrageous medical bills where a guy needed dialysis and his wife started calling to try to find out which dialysis center was in network for their insurance. They lived in Montana so there were, like, two dialysis centers in the entire State. The center he went to wouldn’t tell them whether they were in network or not, or how much they would charge for dialysis treatments. His wife, who is researching this, is a physician herself. So, he goes and gets dialysis because he will die if not. The center, post treatment, they discover, is not in network, and bills them $500,000 for the course of treatments. A half million dollars!
Now, lets look for a solution to this problem. Suppose Congress passes a law that says there is a cap of $2,000 that you can charge for a procedure – and that is the total maximum regardless of the number of entities involved – if you can’t or don’t tell them whether everyone involved in the procedure is in network and ballpark the total cost prior to providing the service. I mean, if you’re going to charge half a million dollars you should be able to ballpark that fee. Not down to the penny, but at least be able to tell the folks within $50,000 what the charge is going to be. If you can’t or don’t do that…you get $2,000 and let it be a lesson to you.
WereBear
So much for Republicans telling us to “shop around.” How far would Wal-Mart (spit) get if they didn’t put prices on anything?
Barbara
@What Have the Romans Ever Done for Us?: Medicare does this. It is the biggest protection that patients have — there is simply a limit that a provider can charge a patient, and that is true regardless whether the person is enrolled in Medicare FFS or a Medicare Advantage plan. The effect of this policy is also to encourage more realistic bargaining between plans and providers for Medicare networks (the most they can get out of network is what Medicare FFS pays). Whereas, for commercial insurance, out of network means I can charge whatever I want, which means that providers can arbitrage opportunistic market power and charge outrageous sums, like dialysis facilities in Montana.
WereBear
I have a new doctor after my old one retired, and he’s innovative and leading towards “systems medicine.”
Why Treating your Symptoms is a Recipe for Disaster
Which is cheaper than stuffing me with prescription drugs to “relieve symptoms” and wait for an organ to fail. Diabetes treatment alone in this country is a disaster that costs billions of dollars and years of suffering.
Zelma
I have two doctors in my family. My son-in-law is a urologist who specializes in cancer and is also on the clinical faculty a UPMC. UPMC is, as Dave well knows, the monster that swallowed the health care system in Pittsburgh. In addition to owning most of the hospitals in the city and having acquired many of the medical practices, it is an insurer and went to war with the local BC/BS. Strangely, for a while, this served to keep prices somewhat under control in the region because the insurer had a motive to keep down medical costs. But this monopoly position is rife with possibilities for price gouging.
My son-in-law works incredibly hard, but is richly rewarded. I believe his income is on the sunny side of half a million. I can’t help but feel that this is excessive.
My grand-daughter is in her third year of a residency in general surgery at UPMC. (This is not nepotism; she was a top student in her medical school class and had other possibilities. It may have made her residency more difficult since the family name is unique enough for the connection to be clear but Pittsburgh is home.)
My son-in-law is not happy with the idea of increased government involvement, although he despises the administrative bloat and the attitude of those in charge.. But my grand-daughter, like many beginning doctors, is appalled by the waste in and cost of the existing system. It’s a generational thing, I gather.
I think that Dave makes an important point that the insurers are not where the outlandish costs are, however excessive their CEO and other administrative salaries are. The problem is the cost of medical services, not the cost of insurance. Until these are brought under control, Americans will continue to pay too much for what is often medical care that is not as good as that in other parts of the world.
LeftCoastYankee
Hi David. One small quibble:
The change in percentage of overall costs would be one time, but the reduction in actual cost would be ongoing. It would be difficult to quantify the savings beyond the first year, but it would result in money not spent every year.
As a former IT data geek I have a developing fascination with the mechanics of data analysis around change impacts (i.e. where an event which can be measured either starts or stops), and how the change is quantified by the experts. Short version: I know enough to make annoying comments and not enough to actually help. :)
Thanks for the blogging!
dr. bloor
@Matt:
Eh. The median is $208,000, which is around what you’d see a fifth-sixth year associate making at a mid- to large-size law firm. Not saying it’s too much or too little, but there has to be some sort of motivating factor for generally smart people to sacrifice a decade’s worth of earning power and going into deep debt.
In any event, I wonder if a better way to think about the cost of labor going forward is “provider salaries” rather than “doctor salaries.” With the continued move toward dishing off all but the tough stuff to PAs and NPs, that cost curve is going to be bent some even if physicians themselves don’t take a big haircut.
Art
IMHO, a lot of the increased costs come in the form of unaccounted for drag. Insurance costs are not the only consequence of the present insurance system. Doctors, those few I’ve talked to, but not necessarily an unrepresentative sample, report they spend a third of their time dealing with insurance companies.
So figure the entire system is operating at %70 of capacity.
Then note that office staff used to be much more limited. Requirements for documentation, approval, and coding required by insurance companies, and accounting to see that neither side is pulling a fast one (That might not be working very well, but still you have to have it.) have slowed everything down,and buried everyone in paperwork. How much is this costing us? WAG = -%25. Figure it is operating at %52 capacity.
But it doesn’t stop there. Delay and selection of sub-optimal treatment options isn’t free. If we had treated it immediately it might be $1000. Ten days later, after insurance has approved, the treatment agreed upon, and a slot opens up in a medical system operating at %52 the cost has gone up to $1300. It is certainly an additional burden on the system. How much of a burden that might be is anyone’s guess.
Of course it doesn’t stop there. Delay in treatment also means poorer outcomes and disability payments, and both doctors and administrators having to make depositions and possibly testifying in a law suit. So there is that also.
And then the lawyers get involved …
In “Murder on the Orient Express” nobody can be effectively charged with murder because each of twelve participated. In the case of Hillary Clinton a great number of people got a dig in and thought it would help them without fatally wounding the assumed unstoppable campaign. Thousands of slights and smears and digs. None individually fatal. But collectively enough to change the outcome.
The US healthcare system is similar in that everyone feels they can get just a bit more out of it and, because it is life and death, the really necessary treatment will be given and bills absorbed. But every one of those slight gougings, and not so slight, create friction and burdens in other parts. Effectively we have a system which costs twice as much but delivers half the actual healthcare. Effective output is by my wild-ass estimation about %25. But very few people seem to be able to do anything about it because it has been slowly deteriorating for so long that it all seems, and I love the phrase:l “customary and normal”.
Barbara
@dr. bloor: Maybe in elite law firms in large markets. The average lawyer makes considerably less than that. And the “average” papers over a very wide range.
jl
I partially agree, and I’ve made similar points on high costs all across a range of real goods and services, besides insurance, as being a big part of the problem. And recommended the late Uwe Reinhardt’s works, one of which is titled ‘It’s the prices, stupid!’
But, important to remember that administrative costs of insurance are not the only costs that insurance chaos imposes. The cost of interruptions and barriers to care caused by sneaky insurance company games and market chaos significantly increases real cost of medical care in the future.
Also, if Medicare for All is given the power to bargain for the prices for a wide range of goods and services, that cuts through a lot of legal and regulatory problems that exist in the US, but not other countries with strong Obamacare type systems, such as Switzerland (Go Swiss! Or go Australia! is my motto. The former is Obamacare done right, and the latter is a strong Medicare for All system, with very highly regulated private insurance along with Medicare for All)
currants
Work doesn’t permit the time to comment when it would be timely, so I’m going to drop this here anyway. Heard an ad on the car radio the other day (Boston MA market) about the cost of medical care, and stopping surprise medical bills. Kept listening to see who was behind it, because it sounded very patient-friendly, for an ad. All I heard at the end was what sounded like a concept, not an org, but lo and behold, it’s an org all right–a PAC called Doctor Patient Unity. And–I’m sure this will SHOCK you–private equity firms are behind the ads. So…about those costs….
Another Scott
@dr. bloor: Dead thread, but I feel compelled to rant a little (not specifically at you, but at the topic).
The Secretary of Defense makes $210,700 a year and manages roughly $760B and roughly 2.9M people. We (as a society) don’t need to pay people really big salaries to get them to do important jobs.
Yes, people need to be able to earn a decent living in return for their investment in education, and yes many professions pay much much more. But money should not be the motivation for being a doctor (or Secretary of Defense). Lots of professions have long periods of training and relatively low pay (artists, post-docs, apprentices, journeymen, and yes residency) – physicians aren’t alone there. And all of these professions have value to society.
I recall that the Bugatti Royale at the Ford Museum was commissioned by a physician. He made pretty good money. ;-)
I also recall that an Iranian grad school friend said that architects and engineers (as opposed to physicians and lawyers) were at the top of the economic and social ladder in Iran. Other countries don’t have the same pay rankings as we do, and there is no reason why the rankings should be static.
Both my J and I have PhDs in STEM and decades of experience. We’ll never see $200K a year as a salary. Too many US physicians really don’t understand how good they have it.
My $0.02
Cheers,
Scott.