The mathematical models are not the only way to make sense of the progress of the pandemic. Raw numbers can tell us a lot too. This is my favorite “how are we doing” set of charts. They can display active cases, confirmed cases, new cases/day, deaths, deaths/day, and recovered, for countries or US states and territories, in linear or log scale, raw or normalized for population. And now they have data by counties, too. Sometimes I just take a quick look, other times, I look for a specific place or parameter, or just more detail. The data come from the Johns Hopkins coronavirus project.
The US is ahead of most countries in confirmed cases (noon, April 8),
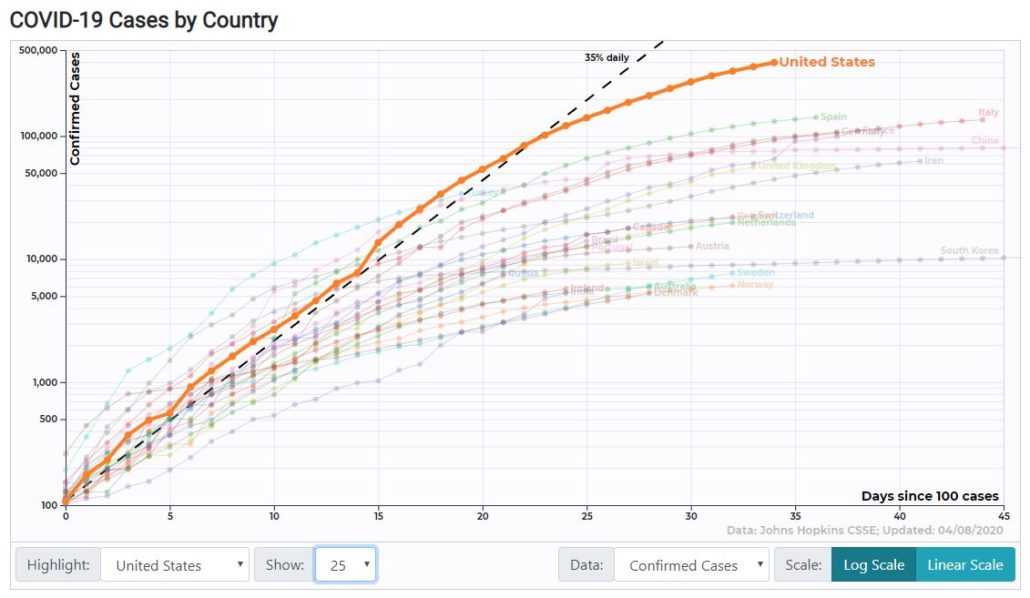
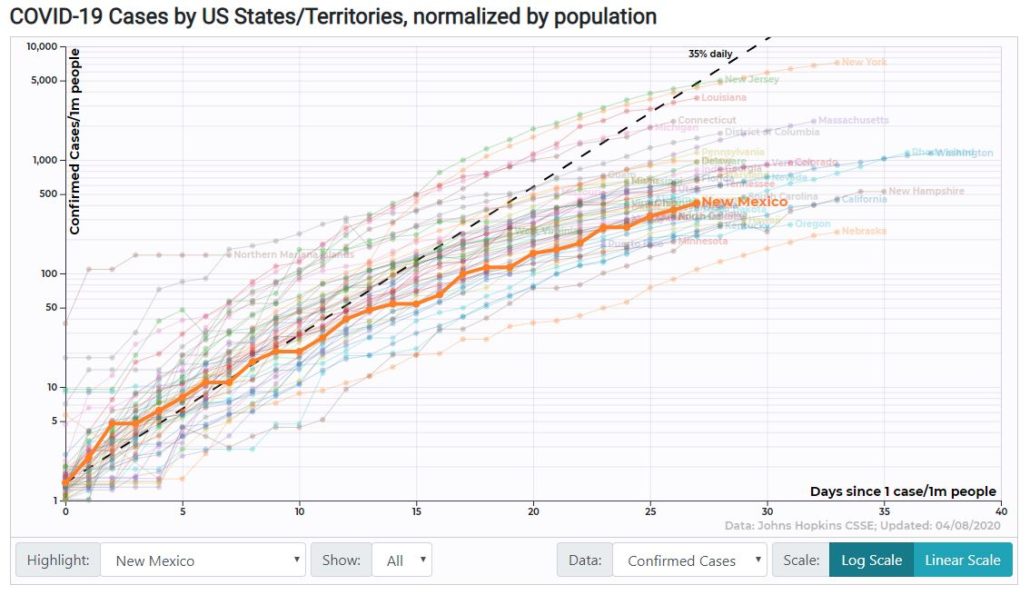
while New Mexico is in the lower half of the pack. I’ve chosen a raw plot and a normalized plot, to show you what’s available.
The Johns Hopkins dashboard is also a good place to get a quick look at the numbers. Again, you can drill down in various ways.
Kevin Drum is posting numbers of deaths for seven European countries, the United States, and Canada. His source is the Johns Hopkins data. It’s another way to get a quick status report. Here is the April 8 report.
If you want to do some tracking of your own, Martin offered simple ways to do it in two posts (one, two).
There are other compilations of data. I recommend that you choose the one you like and stick with it. They have different ways of collecting the data, so switching back and forth may be confusing.
I should say here that all of the data are wrong. All have limitations, all are subject to their own types of error. It’s more important to look at trends than specific numbers.
Here’s a simple explanation of models, a little different than what I’ve been saying. Courtesy of one of our jackals, I think.
Cross-posted at Nuclear Diner
Matt McIrvin
One thing that comes out is that, normalized by population, the US is doing pretty badly but not worst-in-the-world-by-huge-margin, as the unnormalized numbers suggest. Cases per capita are on track to match Italy, deaths per capita on track to match Switzerland. Of course, that is just going by confirmed cases, and it might not mean much because of geographic variation. New York is absolutely one of the worst-hit places in the world, maybe the worst.
I suspect that on the whole the US is comparable to all of Europe, which makes sense since in both cases there is not really a central authority running things.
MisterForkbeard
I’m not sure I understand the last graph (I feel like I’m missing something very basic that I’d understand if I just had time to read through this whole thing).
The last graph indicates that the US is doing better than all other developed countries on a per-capita basis, and the previous graphs describe that the US is doing worse than many other countries on the trend lines in terms of absolute numbers. Is that correct?
Kent
There are endless ways to watch the data. One thing I’ve been doing is watching my own Washington State. At the start of this outbreak, Washington was #1 in both number of cases and deaths. It was also the first state to start implementing social distancing measures. Since then Washington has been constantly sliding down the list of states. Three days ago we were in 10th place among states for number of cases. Two days ago we were passed by both Texas and Georgia and are now in 12th place. CT numbers are accelerating and by the end of the week we may drop another spot into 13th place. This is a consequence of keeping your rise to 5% or below on a daily basis while other states are up in the 10-15% range.
In point of fact, states are really the wrong metric to use when watching this anyway. The virus follows population centers, not state boundaries. In WA it is really a Puget Sound outbreak, not a statewide outbreak. Seattle has a crisis, not Spokane or Vancouver. Same thing in New York. It is a NYC outbreak, not a Rochester or Buffalo outbreak. But laws and measures are implemented by states so we follow states.
ziggy
But, we could have been Canada…
Kent
Exactly so. The US has large intense outbreaks in several metro areas like NYC, New Jersey, New Orleans, Detroit, and Chicago. But it doesn’t have widespread intense outbreaks across the entire country.
In terms of population and geographic extent, the US is really more comparable to the EU. Or perhaps the EU minus Germany. If you added up Spain, Italy, France, Greece, Netherlands, Switzerland, Belgium, etc. and compared the sum EU total to the US our total numbers don’t look quite so bad.
That may all chance in the weeks to come if the outbreak really accelerates in all the big sunbelt cities like Dallas, Houston, Phoenix, Atlanta, Charlotte, Orlando, etc.
MisterForkbeard
@Kent: I’ve seen similar concerns about States v Population centers.
The shape of the disease is vastly different in California: LA vs. Bay Area vs. Northern CA vs. Eastern CA all have vastly different infection characteristics.
rikyrah
Update
A friend of mine’s daughter admitted to the hospital day before yesterday. Has underlying health issues ( asthma). Postal worker. Had a lot of the symptoms.
Got her tests back: it’s only pneumonia.
I cried when my friend texted me.
What kind of world are we living in, When a diagnosis of pneumonia is now met with,
” Thank you, Jesus. “??
Emerald
Let’s remember that the numbers are going to be pretty well skewed in our favor (goodly) because we don’t have nearly enough tests as the other countries. Ergo, our numbers are certainly lower than they would be if we had access to enough tests.
Which is why the shitgibbon is going to pull the plug on federal support for testing. He wants those numbers as artificially low as he can get them.
Wapiti
@rikyrah: Keeping my fingers crossed for you and your friends.
otmar
FYI, the go-to page for statistics on Austria is here.
Things look pretty good, especially the numbers of patients in hospitals are stable. (And we’re far from running at capacity)
After Easter, there will be the first set of re-openings. We’re moving from the hammer to the dance phase.
I really wish that the antibody tests were available in good numbers and quality.
Kent
Which is ridiculously counter-productive to his other aim of opening up the country. The only scenarios in which a country or state can start loosening up restrictions and jump-starting the economy again is with near universal testing.
These people are just too stupid for words. It is just beyond belief.
MisterForkbeard
@rikyrah: I have a mild form of asthma – until about a year ago I didn’t even bother keeping an inhaler. My five-year-old daughter has had pneumonia twice and seems kind of susceptible to it.
I’m worried about myself, but I’m MORE worried about her. At this point if either of us got sick and it came back positive for pneumonia I’d be crying in relief.
Barry
Given the blunders and criminality around testing for the USA, deaths are a less bad measure.
BTW, the Financial Times has charts, free and updated daily:
Coronavirus tracked: the latest figures as the pandemic spreads | Free to read | Financial Times
Yutsano
@ziggy: If the US goes to Hades this November I’m all about starting a petition to join Canada. We can resolve the Oregon border dispute in a more sane fashion.
JCJ
Perhaps this article from TPM was mentioned earlier, but the number of excess deaths over those expected is interesting (and frightening)
https://talkingpointsmemo.com/edblog/this-is-very-important-from-italy-please-read
Another post today at TPM regarding excess deaths in Madrid
cain
@Kent:
This is also why we have a lot of folks in rural areas unhappy since they don’t have as large of outbreaks and remote areas are already naturally distanced. It creates a lot of hardships there.
I personally would like to see us be less hard assed about it for rural areas provided that they keep social distancing and an understanding that they will not be prioritized when it comes to ventilators and the like. (they can’t have their cake and eat it too)
patroclus
Well, I took statistics at the graduate level and I understand what many are saying about the U.S. not being so bad if you analyze per capita and if you discount the fact that emerging market countries don’t have testing or sophisticated public health authorities that can (and do) report accurate statistics. But, the U.S. just had its highest death day yet, we have 1/4 of all reported COVID-19 cases and 1/6 of all deaths. And both those percentages have been going up. We’re already past 4 9/11’s worth of deaths and we seem headed for 10 9/11’s worth (or more). I think the situation is terrible and we have no coordinated national strategy as yet; combined with no real therapies, mass shortages of PPE, gloves and other vital materials, no vaccine and no method of dealing with this other than social distancing. Yes, there have been silver linings and rays of hope about the curve being flattened, but it remains a very dark cloud and virtually nothing on the horizon about the problem being “solved.”
Roger Moore
@MisterForkbeard:
That’s about right, though we aren’t doing better than Canada or Germany on a per capita basis.
Baud
@Roger Moore:
I assume the virus’s spread in the U.S. will be more of a slow roll than in Europe because of our lower population density.
Matt McIrvin
@Kent:
Or with just not testing at all and covering up all the deaths.
Roger Moore
@cain:
This is wrong, though. Rural areas have been less hard hit so far because the virus didn’t get there as fast, but experience so far is that it spread through rural areas just as readily as through cities once it arrives. People in rural areas a more physically spread out, but being physically close together isn’t that big a deal; it’s social distance that matters. Almost all the restrictions we have here in the USA are about social distance. We aren’t locking people up in their houses, just keeping them from congregating.
Robert Sneddon
@Baud: Absent a miracle cure then by the late autumn 2020 about 60% to 70% of the world’s population will have been exposed to coronavirus, the so-called herd immunity level. Being in a remote or thinly-populated area like the mid-Western US won’t stop coronavirus spreading, that just delays it and maybe slows its spread down. What is needed is for any given area to have that 60%-70% of exposed and recovered people who have developed some immunity, that will push the R0 figure way way down well below 1. Saying that, having a mild form of the disease from exposure may not infer proper immunity, research is ongoing on this in many places around the world.
Testing and contact tracing helps but it doesn’t stop the spread, at best it slows it down. That’s all we can do right now, stretch out the medical support that can save a life that would be lost, support and treat someone who would otherwise come out of hospital with irreparably-damaged lungs for the rest of their life.
eric
@Robert Sneddon: and refine treatment protocols. I think this is a big piece of stretching the curve and delaying the second spike. If there is time for the medical profession to assess treatment performance, the second wave can be less deadly.
Roger Moore
@Robert Sneddon:
I think slowing the spread is more advantageous than you make it out to be. It’s not just about keeping the peak low enough that we don’t overwhelm the medical system; it’s also about giving us more time to develop a vaccine and/or testing anti-viral drugs that will make it less lethal.
Doc Sardonic
@Kent: Will try this again apparently fat fingered my email…. As a resident of the Central Florida, Orlando is a concern, but since Orange County clamped down fairly quickly and the large disease vectors ie. theme parks are completely shuttered, hopefully things will be okay. Bigger concern for my area is The Villages. If it hits there and the spread follows the residents normal proclivity for STD spread my area will be a hellscape. Our hospitals have a load problem even during snowbird season…not to even mention a pandemic.
Another Scott
Thanks for this.
The graphics at the JH page are great, but I find it hard to use. E.g. it’s great to know that some county in MS has 0 deaths, but why not make it really easy to see total cases/tests/deaths by state (and how the state numbers change over time)? (Maybe it’s there, but I haven’t figured it out.)
I typically pay more attention to the https://www.worldometers.info/coronavirus/#countries page. We need to do much, much more testing (as everyone knows) to have a decent understanding of where we are and where we’re going. Iceland has done over 90,000 tests per million. The US has done 6,6474 (less than Belgium). Grrr…
We’re flying blind and most of the instruments aren’t working. :-(
CalculatedRiskBlog estimates we need 300,000 tests per day to have a decent understanding of where we are. We’ve been mostly stuck at ~ 125,000-150,000 with ~ 20-25% positive (that needs to be < 5%).
https://www.calculatedriskblog.com/2020/04/april-8-update-us-covid-19-test-results.html
There's no obvious sign of urgency in addressing the real issues from the federal government. It's criminal.
Cheers,
Scott.
Fair Economist
@Another Scott: 300,000 is now far too little. Extrapolating from the number of people who must have been infected 3 weeks ago, even assuming a Washington-like growth rate, we must have millions infected, which will produce hundreds of thousands infected every day. We need millions of tests per day right now to know what’s going on.
Robert Sneddon
@Roger Moore: We (i.e. the world) don’t get a workable safe vaccine until next year at best. We won’t be able to make several billion doses to inoculate everyone who doesn’t have acquired immunity for a long time after that.
Coronaviruses generally don’t respond to antivirals so there’s no existing drug regimen that can be conveniently adapted to fight off the effects of coronavirus and/or reduce the viral load within a body. Some off-the-shelf candidates such as Favipiravir are being tested but it’s going to take until the late summer before it’s known whether they do any good and by that time we’ll be close to that herd immunity level.
One possible pre-vaccine treatment is to process blood plasma from infected and recovered blood donors and extract antibodies but that’s rife with problems and may not work for a lot of people anyway.
Roger Moore
@Another Scott:
Understatement of the thread. The government is not simply failing to address the problem of undertesting; they’re actively eliminating some testing to make the problem worse. Trump apparently believes that if nobody knows how bad COVID-19 is, it will go away.
Kent
I didn’t list Orlando because I thought it was particularly vulnerable. I was just listing random big sun-belt cities in GOP states that have dragged their feet on social distancing. New York, New Orleans, and Detroit were the first places it really escalated. But I expect there will be others in the weeks to come, especially in places that aren’t taking it seriously (mostly the south and GOP plains states).
Kent
Also let the hospitals catch up in terms of PPE and just gain experience in treating this virus. One assumes there must be learning happening in terms of best practices for keeping patients alive even absent new drugs. I’d rather be treated by a hospital ward with 4 months of coronavirus experience under their belts than one that is newly overwhelmed by the disease.
We are already seeing doctors going public with new methods and approaches and information every day. Not just the hydrochloroquine stuff.
cain
@Roger Moore:
Noted. But I think if we put in rules of not congregating they can still go about their business.
We’ll know soon enough if rural areas are going to get infected.. plenty of time left to observe. Of course, with no testing it will be hard to gauge.
EmbraceYourInnerCrone
@Roger Moore: Rural areas also have fewer hospitals and fewer ICU beds. And further to travel to get to the hospital since many hospitals in rural areas have been closed, which means by the time you are sick enough to call an ambulance or go to the hospital it’s going to take longer to get there.
Roger Moore
@cain:
Not so much. There are already rural outbreaks, and COVID-19 spreads just as readily in rural areas as in cities once it gets there. This is not exactly news. For example, the first big outbreak in Colorado was in a mostly rural county that is home to a bunch of ski resorts. Once some jet-setter brought it there, it spread rapidly among the locals.
EmbraceYourInnerCrone
@Doc Sardonic: It’s already spreading in The Villages:
The Vilages see spike in new cases this week
ziggy
@Roger Moore: Another thing we can do with slowing the spread–keep the more vulnerable, older people safe. That way, the younger ones can acquire it, hopefully provide some herd immunity, and keep deaths down. It will be very interesting to see what it looks like when widespread antibody testing can be done.
ziggy
I’m curious how/where you got that information?
Another Scott
@Another Scott: I just played around with the JH map some more. I see that they answer many of my complaints above.
E.g. On the list of countries on the left, notice it says “country/region/sovereignty. Click on United States.
At the bottom of the list on the left you’ll see “Admin 0”. Click the right arrow and it will convert to States and show Admin 1. Click the right arrow again and it will convert to Counties for the highlighted state. In each of those Admin groupings, it gives the types of numbers you’d be interested in.
Well done.
Cheers,
Scott.
Kent
Rural folks drive in to shop at Wal-Mart, Costco, Target and Home Depot just like everyone else. No reason to think it won’t spread in rural areas.
Robert Sneddon
@ziggy: There’s no way to stop the spread of the COVID-19 virus, it appears to be very communicable. There are a few noted examples — for example about a month ago in the US a church choir of about 60 individuals met for a few hours to practice in a hall together, afterwards 45 of them came down with coronavirus contracted from maybe two individuals as the initial vector. At the last report two of the choir members had died from the disease.
It may be possible for individuals to avoid contracting the virus but that means personal isolation and quarantine for months, not just stay-at-home plus shopping occasionally for a few weeks. The current isolation orders are something that is intended to slow down the spread, not stop it spreading entirely.
“Herd immunity” kicks in when a lot of people have had COVID-19 and have gained at least immunity to it. They have a very low probability of catching it again and producing more virus particles to contaminate other people. Anyone who does have it can’t spread it to lots of people who will in turn spread it to others. The measurement is called R0 (R-zero, the replication rate). With R0 less than 1, with fewer susceptible people around the epidemic dies away.
The epidemiologists agree that herd immunity for this disease is about 65% or so but that has to be worldwide, either that or countries where the epidemic has died down will have to close their borders hard like many countries did in the early days but keep them closed for a year or more or until there’s a workable vaccine and most of the vulnerable population of the entire planet has been vaccinated.
Another Scott
@Robert Sneddon: To elaborate:
As long as there’s still exponential growth of cases, the whole population will eventually be infected.
https://ourworldindata.org/coronavirus#the-growth-rate-of-covid-19-deaths
According to another page there, the US is presently doubling confirmed cases in 8 days (it was 5 days a few days ago – so there’s been some progress (but not enough)).
Cheers,
Scott.
ziggy
@Robert Sneddon: Yes, yes, I agree with most of your points, but,
–65% seems like a rather low number for herd immunity, for such a contagious virus. I would expect it to be more like 75% or more.
–where do you get the timeline of late autumn for having herd immunity? At the rate it is spreading (after lockdown), that seems quite fast, and I don’t see an appetite for letting it spread faster.
Robert Sneddon
@Another Scott: It isn’t exponential, it’s a distorted shape that initially begins looking exponential but changes as time moves on. Basically the virus starts to run out of uninfected and non-immune targets and that slows things way down – at the moment a single person suffering from coronavirus can infect three or four people, maybe more on average because most people they encounter are not immune. A few days later four people are passing on the disease, four days later it’s 16 and so on so from one case maybe twenty people get infected in a week.
Once it gets to the point where half the targets or more are immune from having had it already, recovered and started producing antibodies to protect themselves against a repeat case then one person might be able to infect another two. Four days later those people infects another two and so on. In a week maybe seven people are suffering from the disease, not twenty.
Herd immunity works with other diseases which we have vaccinations for, like measles which is a lot more contagious than coronavirus — I’ve seen the R0 for measles described as 15 or more. We need 90% plus immunity, usually gained from vaccination to avoid massive measles outbreaks. The only good thing is that when measles clusters develop in anti-vax cults they don’t spread widely since most folks aren’t stupid and are vaccinated against it.
Robert Sneddon
@ziggy: The herd immunity inflection point AIUI is roughly the time when the rate of new infections matches or falls below the rate at which people are being discharged as “cured”. At that point it’s downhill, the number of cases occurring will decrease significantly but not reach absolute zero.
We have a long way to go still. Without the stay-at-home message the world would now be at ten million confirmed cases and accelerating, lots more dead people and broken medical systems unable to keep treatable cases turning fatal. Left to its own devices coronavirus would reach R0 less than 1 by July with tens of millions of deaths, possibly a hundred million. Stretching it out it will probably take until November before we reach the herd immunity point assuming we stay at home and wash our hands and if we’re really diligent we might only have five million dead total. I am no expert though.
Inspectrix
I am really enjoying this thread. I find my states’s health department data frustrating for listing cases by county. Half of the state is a greater metropolitan area with the most distant suburbs in an adjacent state. Quiz: what state am I in?
I also follow the new deaths/day as the best way to monitor disease incidence. When I can find it, I also want to know new ICU cases and new hospitalization cases. These patients are more likely to be tested and counting severe disease seems more reliable because it is unlikely to go undetected. Trying to count asymptomatic or minimally symptomatic cases is unreliable without widespread availability of rapid turnaround testing supplies.