
(CROI = Conference on Retroviruses and Opportunistic Infections. This is mostly for Dr. Fauci’s crucial work on AIDS/HIV immunology, but it’s nice to know he’s got defenders…)
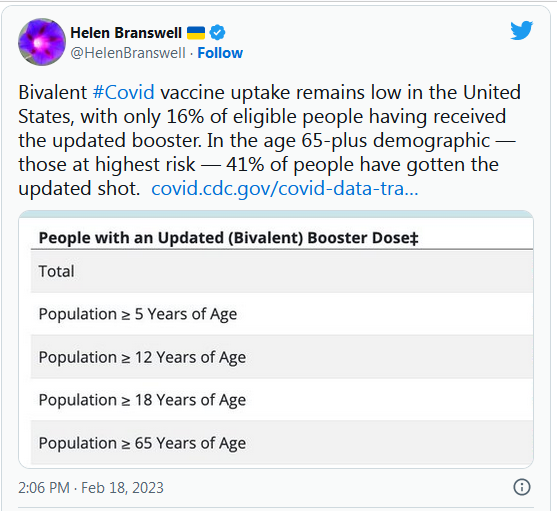
Everyone 6 months and older should get the updated COVID-19 vaccine to stay healthy and protected.
Go to https://t.co/sohfL3zYQA to find a vaccine provider near you.
— Kamala Harris (@KamalaHarris) February 18, 2023
Whatever the epidemiological facts, the world’s moved firmly into ‘living with covid’. Which means we’re going to see much, much more research about living with long covid:
The future of #LongCovid: This emergency is not about to end https://t.co/gUk8rUVgrp
— delthia ricks ?? (@DelthiaRicks) February 14, 2023
In the early spring of 2020, the condition we now call long COVID didn’t have a name, much less a large community of patient advocates. For the most part, clinicians dismissed its symptoms, and researchers focused on SARS-CoV-2 infections’ short-term effects. Now, as the pandemic approaches the end of its third winter in the Northern Hemisphere, the chronic toll of the coronavirus is much more familiar. Long COVID has been acknowledged by prominent experts, national leaders, and the World Health Organization; the National Institutes of Health has set up a billion-dollar research program to understand how and in whom its symptoms unfurl. Hundreds of long-COVID clinics now freckle the American landscape, offering services in nearly every state; and recent data hint that well-vetted drugs to treat or prevent long COVID may someday be widespread. Long COVID and the people battling it are commanding more respect, says Hannah Davis, a co-founder of the Patient-Led Research Collaborative, who has had long COVID for nearly three years: Finally, many people “seem willing to understand.”
But for all the ground that’s been gained, the road ahead is arduous. Long COVID still lacks a universal clinical definition and a standard diagnosis protocol; there’s no consensus on its prevalence, or even what symptoms fall under its purview. Although experts now agree that long COVID does not refer to a single illness, but rather is an umbrella term, like cancer, they disagree on the number of subtypes that fall within it and how, exactly, each might manifest. Some risk factors—among them, a COVID hospitalization, female sex, and certain preexisting medical conditions—have been identified, but researchers are still trying to identify others amid fluctuating population immunity and the endless slog of viral variants. And for people who have long COVID now, or might develop it soon, the interventions are still scant. To this day, “when someone asks me, ‘How can I not get long COVID?’ I can still only say, ‘Don’t get COVID,’” says David Putrino, a neuroscientist and physical therapist who leads a long-COVID rehabilitation clinic at Mount Sinai’s Icahn School of Medicine.
As the world turns its gaze away from the coronavirus pandemic, with country after country declaring the virus “endemic” and allowing crisis-caliber interventions to lapse, long-COVID researchers, patients, and activists worry that even past progress could be undone. The momentum of the past three years now feels bittersweet, they told me, in that it represents what the community might lose. Experts can’t yet say whether the number of long-haulers will continue to increase, or offer a definitive prognosis for those who have been battling the condition for months or years. All that’s clear right now is that, despite America’s current stance on the coronavirus, long COVID is far from being beaten…
Ignominy.
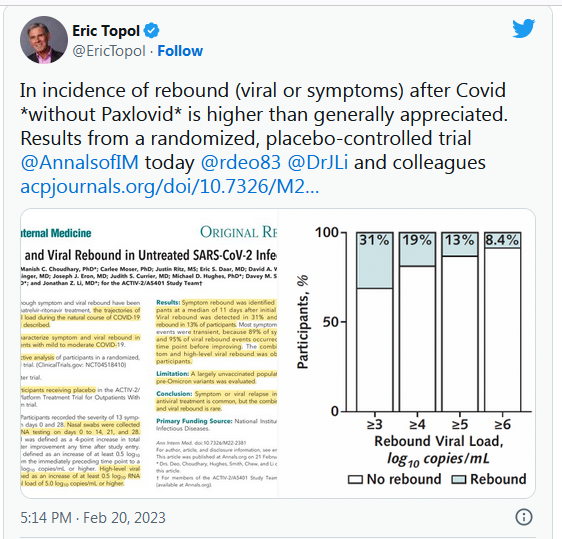
From https://t.co/JzZFPPUbwp pic.twitter.com/8luYZ6ExJi— Eric Topol (@EricTopol) February 17, 2023
======
The next two articles are not precisely coronavirus-related, but they’re useful reading in regards to how much ‘we’ haven’t learned from the last three years:
Governments should invest in vaccines for all strains of influenza virus that exist in the animal kingdom as an insurance policy in case of an outbreak in humans, the incoming chief scientist at the World Health Organization said on Monday. https://t.co/B4BFQ5ckCx
— Reuters Health (@Reuters_Health) February 20, 2023
Pathogen Sharing: Pandemic Accord Could Offer Solutions Or Further Tangle The Web Of Confusion – Health Policy Watch https://t.co/iftmUJPJge
— Global Health Observ (@GlobalPHObserv) February 18, 2023

(link)
Japan 🇯🇵 Covid cases & deaths 21st February (Daily)
Number of newly confirmed cases
19,202 casesCompared to the previous day
+ 12,174 cases+ 72 New Deaths
71,809 Total Covid Deaths#Coronavirus #COVID19 #SARSCoV2 #Japan pic.twitter.com/QeTROOeemo
— Tigress (@tigresseleanor) February 21, 2023
======
Re #LongCOVID "current diagnostic & treatment options are insufficient, & clinical trials must be prioritized…Additionally, to strengthen long #COVID research, future studies must account for biases and SARS-CoV-2 testing issues…"https://t.co/QkBYCTNhrg pic.twitter.com/bR6znu1al3
— Laurie Garrett (@Laurie_Garrett) February 20, 2023
Nearly all Paxlovid drug-drug interactions can be circumvented by holding the drug or reducing its dose. A quick and practical summary @JAMAInternalMed https://t.co/Fi3Vmxn9fY
— Eric Topol (@EricTopol) February 20, 2023
#Covid adversely affects the heart. New research to be presented this wk at the Biophysical Society meeting in San Diego to show Covid raises cardiac risks by 55%. Problems include:
-Arrhythmias
-Myocarditis
-Oxidative stress
-Heart attack
-Blood clots https://t.co/Pfx2L0wslG— delthia ricks 🔬 (@DelthiaRicks) February 19, 2023
(link)
I just finished a book on the history of polio. It made me think of some interesting contrasts and similarities vs #SARSCoV2 pic.twitter.com/wDlWaeU0zR
— Eric Topol (@EricTopol) February 19, 2023
Here is the article from @JACCJournals
Impact of Vaccination on Major Adverse Cardiovascular Events in Patients With COVID-19 Infection
Partial and complete vaccination is associated with a lower risk of MACE (major adverse cardiac events) after SARS-CoV-2 infection. pic.twitter.com/VddFcpnQI6
— Ruth Ann Crystal, MD (@CatchTheBaby) February 20, 2023
======
The coronavirus continues to kill about 2,000 Americans each week. @WmBrangham spoke with @PutrinoLab about the millions who now suffer from the chronic condition of long COVID. https://t.co/x2wbLMyl6O pic.twitter.com/uFvG5JK29I
— PBS NewsHour (@NewsHour) February 16, 2023
Right on cue:

(link)
(link)

(link)

 On The Road – way2blue – Lamu, Kenya in 2021, 5 of 8
On The Road – way2blue – Lamu, Kenya in 2021, 5 of 8Reader Interactions
40Comments
Comments are closed.
NeenerNeener
Monroe County, NY:
121 new cases on 02/17/23.
123 new cases on 02/18/23.
98 new cases on 02/19/23.
53 new cases on 02/20/23.
Deaths at 2186, only up 3 from last week. This is encouraging!
Hospital beds: we’re down to 4% available now, including 9 ICU beds (a loss of 3 from last week) among 4 hospitals. The largest hospital still has no regular available beds.
Matt McIrvin
@NeenerNeener: One thing I’ve learned from watching the local COVID stats over the past few years is that my county was always lamentably short of ICU beds in the first place, COVID or no.
It’s hard to tell because the reporting is so spotty, but it looks like we might have finally passed the peak of deaths from our winter wave. The peak death rate was maybe a third of the 2021-22 winter Omicron wave; that ratio’s bigger than it was in most of the country.
Matt McIrvin
I do wonder exactly why this winter wave hit New England so much harder than just about everywhere else. I suspect the main reason is that XBB.1.5 peaked early here and was by far the dominant variant through the holidays and after. It’s still less dominant in the rest of the country, and that makes me wonder if the US outside of New England is in for worse outbreaks down the line.
Amir Khalid
Malaysia’s Ministry of Health reported 167 new Covid-19 cases yesterday, for a cumulative reported total of 5,041,174 cases. 160 of these new cases were local infections; seven new cases were imported. It also reported one death, for an adjusted cumulative total of 36,957 deaths – 0.73% of the cumulative reported total, 0.73% of resolved cases.
9,663 Covid-19 tests were conducted yesterday, with a positivity rate of 1.4%.
There were 9,330 active cases yesterday, three fewer than the day before. 338 were in hospital. Nine confirmed cases were in ICU; of these patients, six confirmed cases were on ventilators. Meanwhile, 169 patients recovered, for a cumulative total of 4,994,887 patients recovered – 99.1% of the cumulative reported total.
The National Covid-19 Immunisation Programme (PICK) administered 955 doses of vaccine on 20th February: 61 first doses, 46 second doses, 310 first booster doses, and 538 second booster doses. The cumulative total is 72,785,916 doses administered: 28,128,945 first doses, 27,540,937 second doses, 16,310,850 first booster doses, and 805,184 second booster doses. 86.1% of the population have received their first dose, 84.3% their second dose, 49.9% their first booster dose, and 2.5% their second booster dose.
J_A
I had my covalent booster the day it became available here in Houston several months ago. I’ve long been expecting guidance on when a new booster is recommended, or whether vaccine boosters for new variants are coming (Omicron is sooooo last year, nobody does Omicron any more), but I see nothing in the media or the CDC info.
does anyone know when are we supposed to get new boosters? I understand a pitiful amount of people got the covalent one, but, at the same time, the fact that there’s too many lazy or foolish people does not mean those of us that want to stay as protected as possible can’t get new boosters
RevRick
I knew a fifty-year old man who committed suicide when he developed acute arrhythmia from long COVID. Early on, COVID deniers would dismiss the severity of the disease, saying it only had a .3% death rate, that since 99.7% survived we didn’t need to take all these public health precautions. But the warning signs about how chronic conditions from the disease could develop were there early on. Lung damage reportedly seen in 60% of those hospitalized.
I suspect we are just beginning to see the long-term effects of this disease. Many will end up disabled. Many will end up with shortened life expectancies.
OzarkHillbilly
Via commentor Stormy Dragon over at OTB comes this jewel:
Bonkers Republican bill in Idaho would make mRNA-based vaccination a crime
It’s unclear if the two lawmakers know what messenger RNA is exactly.
Stupid is as stupid does.
OzarkHillbilly
@J_A: I think right now it’s once every six months but there is talk of once a year, maybe combining it with a flu vaccine.
YY_Sima Qian
On 2/18 the China CDC provided a summary of state of the COVID-19 pandemic in China as of 2/16:
As of 2/13, ~ 3,491.775M vaccine shots have been injected in Mainland China, 1,310.361M individuals (or 93% of the total population) have taken at least 1 shot, 1,276.858M individuals (or 90.6% of the total population) have completed their primary courses, & 827.102M individuals (or 58.7% of the total population) have taken a least 1 booster shot. Among the > 60 y.o. cohort, 241.673M at least 1 shot, 230.28M individuals have completed their primary courses, & 192.669M individuals have taken at least 1 booster shot.
Taiwan, Hong Kong & Macau do not appear to be publishing daily data dumps, so I am using data from Worldometer.
On 2/20, Hong Kong reported 144 new positive cases & 3 new deaths. There have been 13,443 total COVID-19 deaths to date.
On 2/20, Macau reported 0 new positive cases & 0 new deaths. There have been 121 total COVID-19 deaths to date.
On 2/20, Taiwan reported 12,047 new positive cases & 44 new deaths. There have been 17,564 total COVID-19 deaths to date.
eclare
@J_A: I got my covalent in September of last year, and I plan to get another in March, six months. No official guidance yet, which is frustrating, but I have seen articles that recommend that schedule.
ETA what Ozark Hillbilly said
Matt McIrvin
@OzarkHillbilly: I think that all the CDC/FDA ever recommended was ONE dose of the bivalent booster, six months after your previous booster. I don’t think they ever issued a recommendation for additional doses of the bivalent booster after the first one. But I’ve been hearing mention of people getting them anyway and having little or no trouble doing so.
eclare
@OzarkHillbilly: Saw that, scary. First we have to travel to get abortions, now we might have to to get vaccines. I think I’m.a half day from southern IL if something like that passes here.
dmsilev
@OzarkHillbilly: I read that article yesterday (as a general note, Ars Technica has had a whole bunch of excellent COVID-related articles). Sadly, deliberate and malevolent ignorance isn’t a crime.
OzarkHillbilly
@Matt McIrvin: I’m not sure where or how often I’ve heard it and it is quite possibly just folks being proactive about their vaccinations, never mind health recommendations.
@eclare: @dmsilev: Pro-Life my ass.
YY_Sima Qian
Thank you A.L. for pivoting the coverage to Long COVID! It is shocking how few people here in China are aware of the risk.
narya
@eclare: @OzarkHillbilly: I’m planning to jump on that train, too, probably early April. I keep hoping they’re doing a further-updated booster, but I haven’t seen anything to make me believe that will happen.
kalakal
On a personal note, now 10 days since Mrs kalakal and I started the symptomatic stage of covid. We both seem to be over it, tested negative yesterday.
We both seem to have gotten off very lightly. The vaccines are wonderful.
Ohio Mom
@J_A: I asked my rheumatologist this when I had my checkup last week. She said nobody knows yet what the vaccine schedule going forward will be.
I’ll ask my internist when I see her this summer but I’m guessing Anne Laurie will end up being my ultimate source.
eclare
@kalakal: Good news!
NeenerNeener
I had my bivalent shot in September, so I’ll be coming up on 6 months in March. I have an MRI scheduled for early April and even with Valium I can’t handle wearing a mask in the noisy tube, so I’d like to know if I should have another booster before then. I see my GP this coming Friday, but he’s a Trumper so I don’t know if I can really trust his advice on COVID vaccines.
Kristine
Got my second booster last month, which I guess was about 2 months too soon.
Still seeing masks here in NE Illinois, mostly on the oldsters like me. Way less than half of folks overall. I would guess less than a quarter. The one time I relaxed a little about wearing one I wound up with stomach flu, so I’ll be wearing one when I go out for the foreseeable future.
eclare
@NeenerNeener: I would get one, but I am very pro vaccine.
kalakal
@eclare: Thank you
kalakal
@NeenerNeener: I’d get one, like eclaire I’m very pro vaccine
Another Scott
@Matt McIrvin: +1
My impression is that the CDC wants to recommend regular updated boosters, but they don’t have the direction and the funding to do so.
CDC.gov:
I’ve gotten all of my COVID-19 vaccinations and boosters at the county health department. Once I asked the tech what to do about my J who apparently had a reaction to the vaccine and has only had the 2 original shots. The tech said that those are the most important and the boosters give incremental protection. “She’s protected.”
That’s a little comforting, but given that this is still a “novel” virus, I like every bit of incremental protection I can easily get.
It’s good that the winter wave has been a small one, but still having 200+ people dying every day from this disease when we (still) have free vaccines is a great shame on the USA.
Hang in there, everyone.
Cheers,
Scott.
YY_Sima Qian
@Another Scott:
I don’t think the tech should be making categorical statements like that. The protection from vaccine shots are measured in percentages, not black & white “protected” or not. Yes, the greatest drop in risk of hospitalization & deaths comes w/ the primary course, but the benefit of having up to date boosters is more than marginal or incremental.
CaseyL
People looking for additional booster shots could check to see if their local pharmacy offers them. I got my last booster in September, and have made an appointment with my pharmacy to get another one next month (for the 6-month interval). There was no muss, no fuss making the appointment online: answer a few questions (some generic, about allergies; some Covid-specific, like whether you’ve had Covid or how long it’s been since your last shot).
I should note that I initially made an appointment for a February shot and, even though it had been less than 6 months since the last one, was able to do so. I cancelled that one and rescheduled, because I didn’t want to get the additional booster sooner than 6 months from the last – I have an overseas trip coming up this summer, and want my immunity to be fresh and sparkling when I go. My point being, the pharmacy didn’t say, “Sorry, too soon: come back later,” but let me make the appointment.
Yutsano
@kalakal: Oh frabjous day!
kalakal
@Yutsano: Thank you!
NorthLeft
Goddamn Mississippi.
There. Someone had to say it.
Two rabbits
I had a second bivalent booster at Costco a few weeks ago. It was five months since my previous bivalent, they didn’t question it. I’m planning a Florida trip for most of March and was hoping to boost protection for that. I checked with a few people I trust, there didn’t seem to be good guidance.
I had looked at the CDC info before deciding. Perhaps I was reading it wrong, but I thought it said you could get another shot if it had been 60 days since the last (unless you were immunocompromised, then 28 days). I took another look at CDC site the following week, all changed, no mention of compromised people, and it said you should wait six months. Lots of comments in the media about poor messaging from CDC at that time. I couldn’t really tell from reading it if it meant get a shot every six months, or get one bivalent shot six months after the others and no further recommendations?
In the end, I went with the guidance from a veterinarian in Tasmania, doing research on Tas Devil facial cancers. Hmmm, that is directly related to Covid, right? :-)
New Deal democrat
@Matt McIrvin: I think you are right about why New England and the Northeast generally suffered a worse winter wave than the rest of the country. Those regions went directly from BA.5 to XBB, while the rest of the country had the *relatively* less transmissible BQ.1 in between.
At the moment, I am interested in two things:
1. Spring 2021 and 2022 had the lowest rates of transmissions and deaths of any season. Will that repeat this year?
2. Since there is no further booster being offered at the present time, will infections, hospitalizations, and deaths rise back towards 2020-21 levels, especially among seniors, in a few months?
In general, we are one full year after Omicron now, and we’ve had a good look at what endemicity is going to look like. I did some back of the envelope math, and iirc I calculated that if current conditions continue, today’s seniors have a 1 in 30 chance of ultimately dying of COVID. Good times!
gvg
@J_A: Currently, unless you are in a special immune compromised catagory, their are no plans for another booster. the assumption is we are going to yearly shots like the flu, but even that is not for certain. This can change if a new varient makes it necessary but so far they haven’t. If you notice, everytime there is a new varient they will mention after a short time that it does not seem to be evading the vaccines. Omnicon did. I think that set the expectation in our minds that others would too. It could have worked like that, but it hasn’t.
I also think they don’t want to SAY this too specifically because they will change the plan if the virus makes them and the public has enough fools who will react as if that makes them “wrong” and make more trouble. Better to say as little as possible so they don’t have to explain changes.
It’s a shame we have so many idiots who don’t understand probability and multiple possible outcome planning.
J R in WV
@OzarkHillbilly:
Because Rep. Nichols is totally a professional virologist with many vaccine patents in her name — right?
Thanks for sharing the stupidity with us Ozark — we hillbillies need to stand together in the face of “urban stupidity” like this. Or maybe Idaho has hills? I recall seeing some back when….
gvg
Did anyone else see the Washington Post story about why the South has lower credit scores than the north across all races and incomes? It concludes the answer is higher medical debt and that not expanding Medicaid under ACA is a major contributor, but not the only one. Worse insurance rates and options also, worse health in general etc. Economically it is costing the rich money they don’t realize in higher interest rates and other costs too. Very interesting to me and the kind of thing I would expect. Misers and ‘Libertarians” and be so stupid. https://wapo.st/3XSe5AH
I hope my gift article link works
tybee
@gvg:
thanks, the gift link works.
Matt McIrvin
@New Deal democrat: I always figured one of the worse-case scenarios was that COVID would simply become the third great killer of elderly people, along with cancer and heart disease. It’s not quite that, since existing vaccines are actually quite effective. But it’s a big one among the rest.
Matt McIrvin
@Another Scott: All I know is, I had 5 shots in me (though the last one was about 4 months in the past) and XBB.1.5 was still pretty damned unpleasant. I wouldn’t have liked to get it with anything less.
Matt McIrvin
@gvg:
I was so angry at DeSantis characterizing the rise of Omicron as “they lied about the effectiveness of the vaccines”. He knows better than that. He’s a lying charlatan who plays dumb.
trollhattan
@J R in WV: Having inspected it my ownself I can attest Idaho is very lumpy. Contains plenty of Bills, as well.
Also guns and potatoes.
The vaccine stance may not go over well with the Mormons, who seem not to push away modern medicine (although, see birth control) and are there in great number.