The Alliance for Patient Access (a combination of drug industry advocacy group and physician advocacy group) released an interesting report early last week. It looked at the denial rates of PCSK9 inhibitors. This is a new class of anti-cholesterol drugs that are targeted at individuals with an unusual genotype and high cholesterol. The drugs are expensive ($14,000 or more) and are not cost effective clinical interventions at current prices under almost any range of defensible assumptions compared to the next best alternative.
They highlight the following chart of denials in Florida. I want to look at something else that this chart implies that is completely tangential to the point APA is trying to make.

What I found interesting was the relationship between the initial rejection rate and the reversal rate. I think this tells us how different payers do their utilization management.
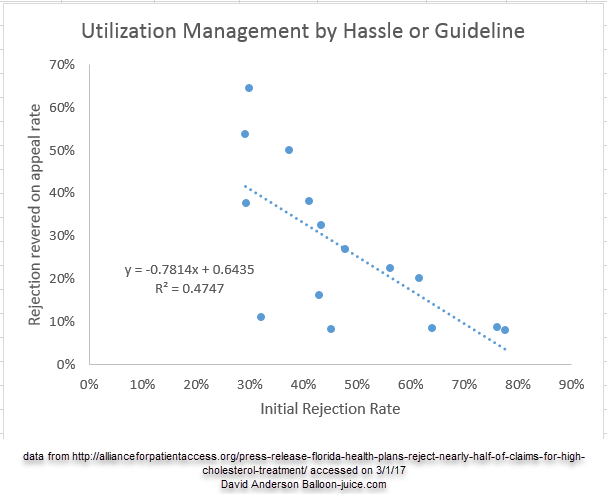
Carriers that have a low initial rejection rate have a high reversal rate on appeal of the initial rejection. Carriers that have a high initial rejection rate don’t lose many appeals of the rejections. The R^2 is high for a simple linear regression as a BS check. More complex trend lines upped the R^2 but for simplicity sakes, a simple fit fits the intuition. Chopping off the top most outlier only slightly decreases the R^2. This is not a comprehensive study, but it is a useful BS check.
So what is going on here?
I think it is a good example of two different utilization management strategy poles. The first pole is effectively utilization management by hassle. A lot of claims will be approved so there will be a low rejection rate. Of those that get rejection, most will get overturned. The utilization management strategy is to create a bureaucratic barrier to use so as to drive people away out of frustration and fear. But if they persist, they get the drug eventually. The side effect of this system is that it could be a subtle selection mechanism to drive people to other plans that are more user friendly.
The other extreme pole is a strict guideline based utilization management system. Most attempts to prescribe will be rejected as the patient does not meet the payers’ guidelines. And since the guidelines are firm, most appeals are also denied. The appeals that do get approved will be ones where the patient’s health status either changes in the course of treatment or there is documentation already in the patient file that was not included in the initial request for authorization. It is a stricter but in some ways a much more transparent process.
Insurers are usually obligated to pay for “medically necessary” treatment. The lawyers will argue long and hard and quite profitably as to what is “medical” what is “necessary” and what is “medically necessary” when answering one way or another means a major swing in expenditures or revenue. Utilization management is partially a systemic way of implementing the insurer’s judgement (constrained by state regulations, medical opinion, and the risk aversion/seeking profile of the legal department) as to what is medically necessary.
Strict rule based utilization management was initially used for the Hep-c drugs. There the rules were often the patient had to be at an advanced disease stage (F-3 or F-4), abstinent from IV drug use and deemed likely to be compliant. These rules were put in place to minimize the number of doses bought at a high price that would not lead to long lasting cures. Over time, the rules have loosened as pricing has come down a bit. The process is clearer than randomly rejecting or approving authorizations and then overturning a significant number of the rejected authorizations. That system no one would know if they qualified. Under a strict rule based system, it is more predictable even if the probable result is a denial.
I would love to see this type of data by carrier for other high cost drugs. I wonder if there is a different set of behaviors for one-off high cost interventions like the Hep-C drugs compared to maintenance medications like these PCSK-9 inhibitors? But until we get this data, it is a good illustration of how different companies manage utilization and thus costs.
AnonPhenom
Former PBM director here. It’s both, hassle and guidelines.
Richard Mayhew
@AnonPhenom: The question is how much of each strategy the different PBMs engage in. FEHB looks to be strong guidelines low hassle while Humana is low guideline high hassle
AnonPhenom
@Richard Mayhew:
Depends on the corporate culture. There are valid reasons to slow walk some of the newer therapies (FDA regulatory capture resulting in the first 18 months of marketing being a clinical trial of sorts) and crappier ones “this is going bust the budget”. Both can be true at the same time.
DHD
Interesting to think that “utilization management by hassle” is basically the thing that American politicians are complaining about when they trot out supposed horror stories of the Canadian healthcare system.
And in the end the only places it really applies up here are primary care and elective surgeries. Ironically, the former is actually a serious problem, while the second is the one that gets harped on all the time by the Republicans and their useful idiots to the North.
Wag
You bring up an interesting contrast between the drugs for hepatitis C and the PCSK9i’s. Hep C treatment is short term, 90 days, with a hard, easily monitored end point of virologic cure, abenefit that occurs in >95% of treated patients.
Compare this to cholesterol treatment with the inhibitors. A patient needs to be treated for life to accrue benefit. And if the model is similar to statin therapy, then treating 100 patients for 10 years will prevent two or three heart attacks. In other words, an insurance company would need to spend $14,000/patient/year, or $14,000,000 to prevent a couple of heart attacks that cost the company $100,000 apiece. All in all, a pretty poor return on investment.
SRW1
Y-axis presumably should say ‘reversed’ and the ‘rate’ may not be necessary.
In any case, the spread of reversals (approx 10% to 65%) for the initial 30% decline rate is amazingly wide.
Another Scott
J deals with this “management through hassle” stuff with our insurance all the time. Her physical therapist doesn’t take insurance, so J has to file the paperwork herself. The “codes” seem to change randomly within the year (in addition to often officially changing annually). Claims that will be approved for months on end will suddenly be denied (for the same treatment), so being “approved” is never the end of it – “smooth sailing from here on – we’ve been approved!!”. Claims that were filed months ago have to be refiled because they “lost” some paperwork. Etc.
It’s maddening, and a huge wast of time (and money) for everyone involved. It’s hard to believe that BCBS is actually saving much money doing this (the claims are roughly $100 each), but it’s been going on for years. I’d hate to actually be one of the 1/1M people who actually need these $500k+/yr treatments.
(sigh)
Thanks.
Cheers,
Scott.
ThresherK
I’ve never heard of ’em but the info that they’re A combination of drug industry advocacy group and physician advocacy group leaves me confused, basically because everything else in this post is over my head.
Allliance for Patient Access: Are they a fair player, or just another “Americans for Health Liberty Freedom and Choice and What Are You A Commie” newspeak-labeled group?
David Anderson
@ThresherK: If you look at their funders, it is entirely big Pharma. Their angle is that anything should be prescribable at any time at any price. That does not sound good coming out of the spokesbots of Pharma but it is convincing come out of a doctor’s mouth.
Barbara
It’s hard to evaluate this without some kind of baseline for rejections/reversals for all kinds of drugs. There can be rejections that are based on things other than UM guidelines. In addition, some of these insurers might actually have this drug as an on-formulary product if certain conditions are met (meaning that you would expect the rejection rate to be lower for this drug all other things being equal). In my experience, probably a little out of date at this point, PBMs are better at communicating formulary status and UM guidelines, as well as having a much higher market share and thus doctors being more familiar with what they have to do to get something covered. This probably explains some of these numbers. For instance, ExpressScripts and CVS received a pretty low number of claims given their overall market share, which might be a function of doctors knowing in advance not to bother. Of course I am speculating — the overall point is that this review is probably not well-enough controlled to say a whole lot about a given carrier’s view on utilization management. Especially since it comes from a highly interested party.
David Anderson
@Barbara: Agreed, it does not prove what the interested party thinks it proves. I found the relationship between the level of initial rejections and the overturned on appeal rates to be fascinating. That I think is something that the author of the original piece would not give a shit about.
Eric S.
After my surgery Tuesday I had 3 prescriptions: percocet for pain, anti constipation and anti nausea to counter the side effects of the percocet. 30 pain pills to take every 4 hours? No problem. Express Scripts only allows me 7 of the anti nausea drugs per month. Fortunately I don’t have that side effect.
Alex
This interests me because it’s the opposite of the pattern you seen with applications for Social Security disability. With SSI and SSDI, they deny more than half the applications, but way more than half of those who appeal are accepted. SS is supposed to be using a strict guidelines approach, but some judges find the guidelines weren’t followed in about 90 percent of appeals. The initial denials discourage people from applying because they know it would take 2 years even if they won in the end ( the hassle factor). And the system further avoids having to pay out because many applicants are so sick they die before they can get their appeal.
Barbara
@David Anderson: Right. Just looking at ESI and CIGNA, they have high rejection rates but low reversal rates. This says to me that they might have some other Hep C product as an on-formulary and clear criteria for when you don’t get that product as a first measure. (There are now multiple Hep-C products.) Those doctors who insist on starting with the off-formulary product are less numerous (ESI in particular), likely to get rejected and unlikely to get that rejection reversed. I realize that in an ideal world all drugs would be cheaper, but in the world that these companies deal with, playing one drug off against another is how they manage to keep prices from spiraling utterly out of control.
ElegantFowl
It struck me today that I haven’t heard anything about the political fallout of medical underwriting, and I wonder what Republicans plan to do about that. I mean, every Republican proposal has some sort of “high risk” plan, and as soon as you use those words you bring back medical underwriting, right? Everyone has forgotten about the hassle and anxiety of pre- and post-coverage questionnaires and exams and denials, and they’re going to bring that all back, and I don’t see how it can be hidden or obfuscated or blamed on Obama. Any idea what the plan is?
ElegantFowl
And I imagine there could be dramatic advances in risk reduction through medical underwriting these days, once that class of innovation is unleashed. Family history, genetic analysis, lifestyle surveillance, social media monitoring, etc. None of it was legal under Obama, all may be legal under Republicans, and people are surely gonna hate it.
EthylEster
Personally I have always revered rejection.