Earlier this week, I presented the following virtual poster at Academy Health’s 2021 Annual Research Meeting (ARM-21). I’m part of a team centered at Duke Margolis and funded by the Kate B. Reynolds Foundation to examine North Carolina Medicaid policy. As part of this remit, we looked at patterns of disenrollment and churn (coverage loss and then fairly rapid regain) for adults from 2016-2018. This poster focuses on Medicaid churn for post-partum women.
Medicaid pays for a significant number of all births in the country. Pregnant women have looser income qualification criteria for Medicaid than most other forms of Medicaid. In North Carolina, a single woman with no kids and in good health can not qualify for Medicaid at any income level. However, a pregnant woman can qualify for pregnancy Medicaid if she earns less than 196% Federal Poverty Level (FPL). This pregnancy eligibility expires 60 days after birth. At this point, a mother will either be moved to a different Medicaid eligibility group such as income based caregiver Medicaid where she can earn up 41% FPL for a family of two (or more) or she is disenrolled.
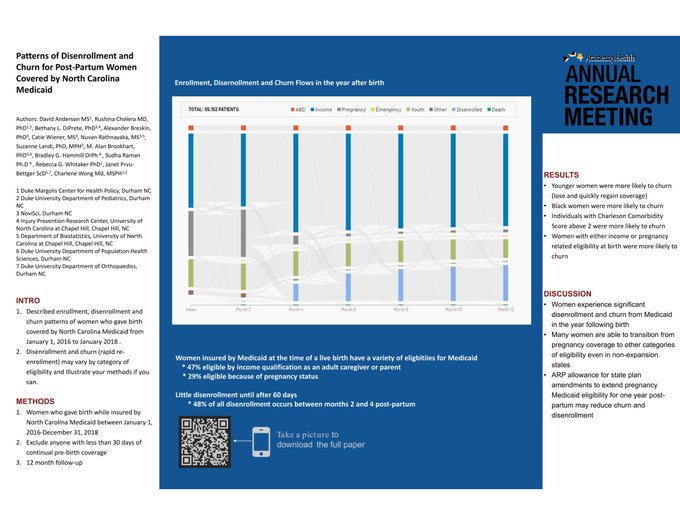
Not every woman who gives birth while insured by Medicaid is eligible via the pregnancy channel. Does this matter for disenrollment and churn?
Yes!
Individuals who gave birth while eligible via the Aged, Blind, Disabled channel had a far lower risk of losing coverage at any point than any one else.
Individuals who were income qualified at the moment of birth have reasonably stable enrollment through the year post-partum.
Individuals who were on pregnancy Medicaid had significant coverage losses at the end of 60 days. Roughly a quarter of these individuals were disenrolled immediately at the end of sixty days. Three fifths were redetermined into the income qualified group.
We then looked at who disenrolled and came back.
Sicker individuals who lost coverage were more likely to re-enroll. Women who were covered in either income or the ABD eligibility groups were more likely to churn.
Why does this matter?
Insurance disruptions are care disruptions. The US has a significant maternal mortality problem. Churn (coverage loss and then coverage regain in a short time period) is likely indicative of administrative frictions rather than true eligibility losses. Fixing churn likely means more people will get insurance that they qualify for. The American Rescue Plan allows states to file a State Plan Amendment to extend the post-partum Medicaid eligibility period from 60 days to 1 year. This likely will reduce disenrollment and churn.
Barbara
The only reason NC covers pregnant women at the level it does is because federal law made pregnant women at or below a certain percentage of the FPL a mandatory coverage group before Medicaid was expanded.
When you say that Medicaid covers a “significant” portion of deliveries, I think you should be more specific. For whatever reason, the data seems to vary based on source, but broadly, the range is between 25% and 70%, circa 2018. To me, it looks like the percentage has gone down in states with lower FPL rates probably because alternative coverage through the ACA has become available, while states with high poverty levels (Louisiana, New Mexico) rely increasingly on Medicaid, regardless of Medicaid expansion. (The percentage FPL for maternity coverage is higher than the 133% FPL ceiling for Medicaid expansion.) The average is just around 43%. Nearly half of all children being born in the U.S. will have the benefit of medical care only thanks to the Medicaid program.
TomatoQueen
“Insurance disruptions are care disruptions. The US has a significant maternal mortality problem. Churn (coverage loss and then coverage regain in a short time period) is likely indicative of administrative frictions rather than true eligibility losses. Fixing churn likely means more people will get insurance that they qualify for. The American Rescue Plan allows states to file a State Plan Amendment to extend the post-partum Medicaid eligibility period from 60 days to 1 year. This likely will reduce disenrollment and churn.”
This happened to my son’s caregiver. Pre-expansion, the Battle of Battles in Virginia, Medicaid coverage had to be re-approved to continue after 60 days, which process was the responsibility of the caseworker: schedule appointment, probably reschedule, interview, copy all documents, pend for missing documents such as the birth certificate as the hospital footprints stopped being an official/acceptable paper years ago, finally get everything copied to the file, run the paperwork, approve, and send the things to Social Security to enumerate. That’s one baby, and to do all that correctly took about 60 days, and holes develop in those cases rapidly. My caregiver’s caseworker didn’t do the first step–schedule the appointment. A year later, her hospital bill still wasn’t covered by Medicaid–the baby was, but not hers. (The reason for the baby’s coverage happening is that hospital social work departments send the baby’s basic record of birth to Medicaid within 48 hours, to let Medicaid sort it out.) Baby was almost two when her mom’s bill was finally covered. Post-expansion, this kind of bullshit doesn’t happen. This is an example of states running Medicaid as they see fit; Florida was just as bad and Connecticut was a little better–but this was Virginia, a bureaucratic black hole. Also, that caseworker no longer works for the agency.
“The US has a significant maternal mortality problem.” Yes it does generally and more specifically among black women. The numbers are hideous and shameful. It is bad enough generally and more than worse enough among black women that the latter needs to be a central issue. My experience with this issue goes back to the early eighties, and it’s no better now. Infuriating.
Barbara
@TomatoQueen:
It is important, however, to point out that maternal mortality and complications among black women is a far bigger issue than insurance coverage. Of course disruption in care contributes to poor outcomes, but the sobering truth is that even the lowest risk (e.g., best educated, most economically stable) black women have worse outcomes than the highest risk white women. That’s a difference that goes way beyond Medicaid churn.
lowtechcyclist
In those states that choose to file such an amendment.
As you said yesterday, we’ve got a huge Give A Damn problem in this country. Especially in some parts of it.
Betsy
Have heard criticisms of maternity and pregnancy coverage mandates as unneeded because being unique to only a subset of insureds. Even saw a letter to the editor arguing that “special” maternity and postpartum coverage shouldn’t be mandated by the Affordable Care Act because people shouldn’t have to pay for what they don’t need.
I wrote a letter to the editor: On the contrary — Maternity coverage is the *ultimate*, in fact that *only*, universal health condition.
What person was not the product of a maternity event?
Barbara
@Betsy: So I shouldn’t have to pay for anyone’s cigarette related cancers? And of course, I should be spared the expense of prostate cancer. The usual basis for whining about maternity coverage is that pregnancy is a voluntary condition, although that would be hard to maintain with respect to the product of the pregnancy, which surely did not chose to be conceived or born.
TomatoQueen
@Betsy: Mitch McConnell.
David Anderson
@TomatoQueen: All cloacas matter
TomatoQueen
@David Anderson: Soooo close. I almost had a new keyboard there.