The cost curve is bending to a lower slope of less cost acceleration.
The Robert Woods Johnson Foundation has released preliminary 2015 results on medical service pricing:
We have observed many times that growth in health service prices remains extremely low, and this month’s trend report suggests that this trend is continuing, reporting an annual increase in health care prices for 2015 of 1.1 percent, the lowest recorded since Altarum’s series began in 1990. Given the flatness of this series, the two drivers of the recent growth in health spending have been coverage expansion and spending on prescription drugs.
In 2015, the nominal GDP growth was 2.9%. Inflation was roughly 1%. Healthcare price inflation was within rounding errors of general inflation. This is extremely important news.
However cost control is not only a matter of price. It is a matter of quantity.
Everyone expected quantity of services to go up significantly. The CBO had projected a spike in GDP devoted to healthcare spending in 2014 and 2015 because it was projecting the US uninsurance rate to be cut in half. Below is a November 2013 chart from the White House that shows how the CBO anticipated a spike:
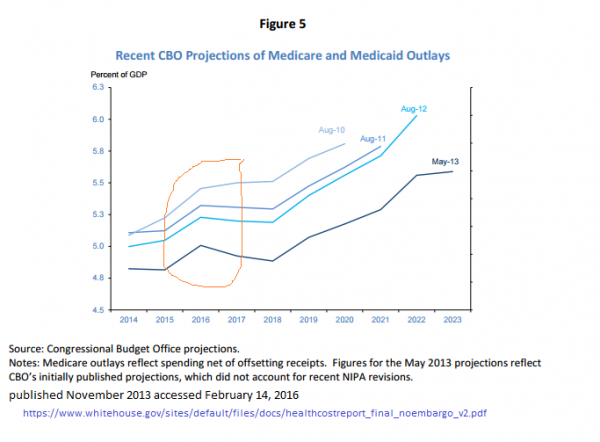
The RWJF research shows that spike shown through the data:
This month’s results are quite consistent with this foreshadowing. The quarterly trend in overall health spending growth using the Altarum Health Spending Economic Indicators series shows a clear peak in Q1 2015 at 6.7 percent, with subsequent declines every quarter. Partial data for Q4 (October and November) show a spending growth rate of 5.2 percent. While overall spending growth in 2015 will clearly exceed that of 2014, a reduction appears to be underway.
Total spending is a function of the average price per service and the number of services being sold. Since we expanded access to health insurance and healthcare with the biggest wave of new entrants to the system happening in 2014 and 2015, the number of services being used should have gone up. They did. Some of that incremental increase was due to “catch-up care“. That wave seems to have crested. The rest of the increment is the “natural” healthcare utilization rate of newly insured people who have had their “gonna kill me now” problems taken care of.
Charles Gaba has argued, the easy large scale additions to the ranks of the insured is complete.
6. The remaining uninsured STILL haven’t a clue about the deadlines and/or tax penalties:
The final factor is one which I’ve written about before, and which there seems to be no obvious solution to: In spite of a massive outreach/marketing/eduction effort by HHS, CMS, HC.gov, the state exchanges, the private insurance carriers, Enroll America, Families USA, Planned Parenthood, the United Way and dozens of other organizations,people STILL had no idea about the deadline and/or mandate tax:
This will change once the large population former Confederate states expand Medicaid at some point in the next decade but there are not big pools of easy conversions readily available.
What does this mean?
The cost curve is bending. If prices can grow at roughly the rate of inflation and not even nominal GDP quite a few long term federal financing problems go from dire to manageable.
OzarkHillbilly
I blame Obama.
Docg
Unfortunately, much of the health insurance being sold to those newly coming into the market is like a new car without an engine. Looks good but is unusable due to impossible copays and deductibles. My doctor recommended a nuclear cardiac stress test, of which my “contribution” would be $3,700. Thanks ever so much. I’ll just die quietly, the real goal of my “Silver” plan.
Richard Mayhew
@Docg: You are an unusual case the typical person getting newly covered via PPACA is getting coverage of at least 87% AV through either Medicaid or CSR Silvers.
The goal is not to tell ppl to die quietly in the corner
CarolDuhart2
As someone who has a chronic condition, one thing you haven’t mentioned is the rise of various care-management programs. Mine is ‘Condition Care” and once a month or so a nurse calls in to help me manage my care. I can mention symptoms, issues with medication, whatever and they help men keep on track.
p.a.
Really? With a redistricting-insured House majority of mouthbreathers in place for the forseeable future? ACA funding isn’t an economic issue, it’s an issue of political economics.
If the D’s don’t get their down ticket house in order the ACA could suffer death by a thousand cuts. The legal challenges have had a modest effect on ACA. The next step, since it can’t be killed outright, is to starve it, cludge up the money flow, make it as inefficient as possible, and blame BIG GUBMINT.
Docg
While it may not be a stated goal, it becomes the functional outcome. Richard, I think you are a caring professional, but frequently get lost in the wonky weeds of health insurance policy. This leads to losing sight of how bad access to medicine overall has become with the excesses of corporatization of its financing and provision. Statistics are meaningless individually, by definition.
rikyrah
Thanks for the info Mayhew.
Eolirin
@Docg: And individuals are meaningless by definition when it comes to setting appropriate national health care policy. No system is going to ever serve 100% of people in the most ideal way. It’s all managing resource allocation to help the greatest number of people the most you can while avoiding the really bad edge cases.
And yeah, there are still systemic copay/deductable problems, and they do need to be fixed. Just like drug prices, medical device costs and specialist procedure costs need to be reduced. But those issues are just as present in the employer provided insurance markets as they are on the exchanges, and solving them is going to take more than just expanding access to insurance. The ACA is not contributing to these issues, it’s simply not going far enough to fix them. This is not a new problem.
Sister Rail Gun of Warm Humanitarianism
@Docg: I’ve also run into insurers targeting certain tests as a poor return on the money. Nuclear stress testing is definitely in that category.
Or your doctor could be charging a lot more than the insurance is willing to pay for it and has no contract to discount it.
SenyorDave
I wonder if this story will even make it into the news. This is, as Joe Biden says, a BFD! My guess is that except for NPR and MSNBC, who might actually have a segment about it, it will be largely ignored. If I were at a town hall with one of the candidates I would ask about, especially with someone like Cruz. It gets back to the whole issue with the GOP, in that once Obama has done something it poisons the well. If Obama personally developed a drug that cured cancer the Republicans would petition the FDA to ban the drug in the US.
NCSteve
And yet, BCBSNC, with its narrow networks and supposedly crushing market power in North Carolina jacked up rates 33-45% last year (I am now officially eligible for the Public Option Lieberman killed, not eligible for subsidies and no silver plan that costs less than 10% of my AGI) and is making noises about getting out of the Exchange altogether because of the losses its been taking.
They claim that the Exchanges have been loaded up with a huge number of very sick people who quit paying premiums as soon as they get treatment (the latter is a thing I doubt makes much difference to their financial positions).
I wish Richard, or someone, would take a look at this because I smell a rat. And the rat I smell smells an awful lot like “hospitals still passing on the costs of treating the uninsured to the insured because of the Medicaid Expansion Massive Resistance plus repeal of the risk corridors but they’re too deep in McCrory’s pocket to say it).”
Mind, BCBSNC isn’t claiming it’s only taking losses on its broadish network policies. It’s claiming it’s taking huge losses on all policies, including its narrow network, get permission before you die waiting to see a specialist policies. Something weird, and possibly a bit crooked is going on here. I don’t know if they’re posturing trying to lever someone into giving them something, if they’re just incredibly inept at calculating actuarial values in a market where they can’t exclude sick people because they never did it before or if the providers have been screwing them ragged all along and they’re just now noticing.
Starfish
@Richard Mayhew: But most of the insurance plans on the exchange are the high deductible ones, and more and more employers are shuffling all their employees onto the high deductible plans too.
Sister Rail Gun of Warm Humanitarianism
@NCSteve: Their CEO flat-out stated that the Medicaid expansion would improve things, so I have a feeling you are definitely smelling that rat from the hospitals.
gene108
@Richard Mayhew:
I do not think 87% AV is high enough for a lot of people to make the premiums, co-pays, and deductibles affordable, from what I see via anecdotal statements in real life and on the Internet.
Sister Rail Gun of Warm Humanitarianism
Also (since I can’t edit) the insurance commissioner has announced an investigation into BCBSNC regulatory compliance. The attorney general has been making noises as well.
Starfish
@gene108: This is the impression that I am getting too. The people who are just scraping by to pay the premiums can’t pay the premiums AND the co-pays AND the deductibles.
TallPete
It sure doesn’t feel like the cost curve is bending. My family premiums increased 30% in Jan. That’s for a high deductible plan – lowest cost plan available on MNs marketplace site.
gene108
@Starfish:
In a functioning government you would find a way to increase the actuarial values of plans based on income.
At the rate people are finding plans unaffordable, in total, there is a simmering backlash brewing.
This is one reason Bernie has attracted so much support with promises of single-payer and what people feel will finally be affordable health care.
p.a.
@Sister Rail Gun of Warm Humanitarianism: In North Carolina? I thought the state gvt there would like nothing better than for any and every aspect of OCare, exchange, Medicaid, whatever, to circle the drain. Good to see there’s some parts of the state’s gvt they haven’t effed up yet.
gene108
@p.a.:
AG is a Democrat.
Mike in NC
BCBS in North Carolina is virtually a monopoly in most counties. I think there is one competitor in the entire state, and our wingnut governor and tea party legislature oppose Medicaid expansion.
Fair Economist
The long-term funding problems were never ‘dire’. Even before Obamacare we could have covered the cost with taxes no higher than your typical European state. Obamacare cut the forecast deficit by 2/3, to about 2% of GDP IIRC, which is absolutely not “dire”, requiring only an adjustment to the payroll tax considerably less than the Greenspan commission. The current improvements are just making an already non-dire problem even more manageable.
I find it frustrating how many people talk about expected healthcare costs as if we were still in the pre-Obamacare situation. We’re not, and it’s been 6 years now.
Remember the whole healthcare “direness” was cooked up as a granny-starving situation. It’s always been the case that if we actually hit the Medicare wall, the olds would just have insisted on raising taxes to cover it. The panic was engendered by anti-tax advocates who rightfully feared their ideology would go out the window when people faced immediate cuts and were trying to get cuts far enough in the future that they could get them through.
Sister Rail Gun of Warm Humanitarianism
@p.a.: The AG wants to know
The Dept of Insurance has had to shift more people to the phones to cope with the volume of complaints.
Kofu
I wish you had been slightly more explicit in your post, about which way the curve is bending. You’re vaguely positive about it, so I infer you mean that it’s bending downwards?
This is the closest you get to saying that:
Richard Mayhew
@Kofu: I will update shortly… In my discussion circles elsewhere “bending the curve” implies downward. Sorry about staying in assumed jargon.
Balconesfault
A friend in the pharma industry was arguing to me the other day that most of the provider side cost curve bending is due to Drs being pulled into larger practices rather than being solo practitioners. Valid?
Richard Mayhew
@Balconesfault: I am suspicious of that explanation as larger practices means, all else being equal, more provider negotiating leverage. I don’t have evidence for or against the theory though.
J R in WV
You all know what this means, don’t you?
Obamacare is a total success, from a medical perspective, from a financial perspective, from a moral perspective.
The Republicans passing bills they claim reject the ACA without replacing it in any way at all over and over is wrong in all those ways, Medically, Financially, and Morally. The Christian thing to do is to care for you neighbor. Now we can care for our neighbor, and cure his illness, or at least treat it to make life more livable.
But the so-called Christian political party wants to repeal the Obamacare act, even though it saves money and lives… how is this possible? Wait, maybe it’s possible because the Republican party isn’t the least bit Christian?!?!
I think I am more Christian, as a non-believer who tries to help my friends and neighbors, than Mitch McConnell is. He doesn’t even know what JC ordered his followers to do with regards to helping one’s neighbors. If he understood the commandments of Jesus Christ he wouldn’t try to repeal the ACA withoug replacing it with an improved and more Christian program.
Doesn’t that sound odd? It does to me. Even placing McConnell in a sentence with Christian requirements to help one’s neighbors is crazy sounding~!