The Congressional Budget Office released their score of the Senate’s Better Care Reconciliation Act (BCRA). It does not include the Cruz amendment. There is not a whole lot of difference since the last score as there are not many large changes on the coverage side.
I just want to pull out a few things. The most important thing to pull out is Table 3 regarding Medicaid:
The largest savings would come from a reduction in total federal spending for Medicaid resulting both from provisions affecting health insurance coverage and from other provisions. By 2026, spending for that program would be reduced by 26 percent (see Table 3, at the end of this document).3
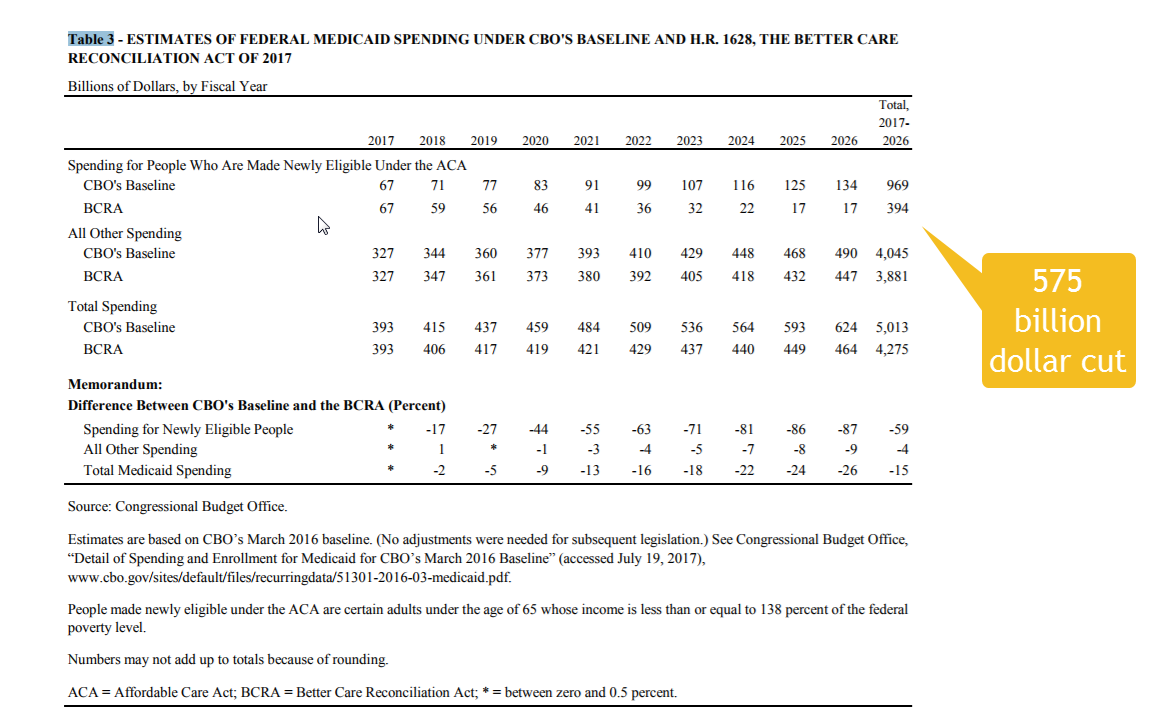
It is a $575 billion dollar cut to Medicaid. Throwing inadequate opioid specific money or allowing for a $200 billion dollar back door CSR funding stream won’t do anything remotely sufficient to address the people who lose coverage because of these cuts.
THe next nugget is a repetition of the basic point that the value proposition of super high deductibles is absolutely atrocious for lower income individuals:
Because this legislation would change the benchmark plan (in part, by repealing the current-law federal subsidies to reduce cost-sharing payments), the average share of the cost of medical services paid by the plan would fall—for the 40-year-old with income at 175 percent of the FPL in 2026, from 87 percent to 58 percent—and his or her
payments in the form of cost sharing would rise. And the person’s net premiums would be higher under the legislation than under current law for plans of comparable actuarial value. Those changes, CBO and JCT estimate, would contribute significantly to a decrease in the number of lower-income people with coverage through the nongroup market under this legislation, compared with the number under current law.
The baseline deductible in 2026 is a mind busting $13,000. This matters a lot for the people who are losing Medicaid. The deductibles are an absurdist joke.
a single policyholder purchasing an illustrative benchmark plan (with an actuarial value of 58 percent) in 2026, the deductible for medical and drug expenses combined would be roughly $13,000, the agencies estimate… Under this legislation, in 2026, that deductible would exceed the annual income of $11,400 for someone with income at 75 percent of the FPL. For people whose income was at 175 percent of the FPL ($26,500) and 375 percent of the FPL ($56,800), the deductible would constitute about a half and a quarter of their income, respectively.
Finally, the CBO notes a clear mechanical problem that can not be fixed without 60 votes:
The limit on out-of-pocket spending in 2026 is projected to be $10,900. (Under current regulations, the limit on out-of-pocket spending is defined by a formula based on projections of national health expenditures.) Therefore, plans with an actuarial value of 58 percent and a deductible of $13,000 would exceed that limit and would not comply with the law unless the formula used to calculate the limit was adjusted. CBO and JCT estimate that a plan with a deductible equal to the limit on out-of-pocket spending in 2026 would have an actuarial value of 62 percent. A person enrolled in such a plan would pay for all health care costs (except for preventive care) until the deductible was met and none thereafter until the end of the year.
The benchmark plan can’t be built.
Oops
TenguPhule
As always, Feature, not a bug with these Republican scum.
Mnemosyne
Kay brought up a magic phrase yesterday that I never seem to see when discussing healthcare: “sliding scale.” Why should a disabled person living on SSDI have to pay the same co-pay as me, a person with a pretty decent job and no income-devouring rugrats?
Any woman who’s gotten services from Planned Parenthood knows that they operate on a sliding scale. Why can’t Medicaid or other government healthcare do the same?
justawriter
I have an interesting data point that I would like to share. For my paper I cover a very small town city council that went with a grandfathered in plan when the ACA was passed. BCBS of ND finally told them there grandfathered plan was going to start jumping to double digit increases every year so they should move to an ACA-compliant plan. The old plan only paid for three preventive care expenses vs. the two dozen or so required by the ACA. The new plan has a slightly higher deductible. However, the kicker is that the city’s premiums will be falling from $11,000 a month to about $10,000 a month. This is one of the untold stories about Obamacare, and I wish there was more info available about what is happening in the Employer Sponsored Insurance market.
rikyrah
The CBO comes through…yeah.
Tell the truth and shine a light on their horror.
Jeffro
Sweet emergency room Jesus, a deductible of $13,000? Can you imagine saying that to constituents – any of them making less than $200k a year, anyway – with a straight face???
Eljai
I just wish the CBO report would spell it out so that certain lazy journalists can’t avoid the implications when they’re reporting on this, i.e., “The largest savings would come FROM KILLING PEOPLE.”
Villago Delenda Est
@Eljai: Specific people. Republican senators.
TenguPhule
@Jeffro:
“It’ll be the fairest, cheapest Healthcare ever, believe it!”
cmorenc
The object of $13k deductible plans is insurance of the sort the supposed target market for such plans wouldn’t be able to actually use nor really afford to buy. The net effect is to largely move the insurance market back where it was pre-ACA, with only the sorts of people who were able to obtain coverage back then able to afford health insurance (or have it employer-provided, but full of the same swiss cheese holes as before).
narya
@Mnemosyne: Actually, there IS government-FUNDED healthcare that requires a sliding fee scale: federally qualified health centers, and the scale has to have several “bands” in it, based only on family size + family income, measured against the federal poverty level (updated each year). Discounts are available to anyone making under 200% FPL, so if you have insurance, the discount would be applied to your co-pay.
Brachiator
@Mnemosyne:
But Planned Parenthood is anathema to conservatives. You cannot compare it to God-approved all American Trumpcare.
mai naem mobile
Meanwhile Cruz himself gets a platinum plan through his wifes employer, Goldman Sachs
The same fuckers who got a nice fat bailout and hide their money offshore when possible so that they don’t have to pay taxes.
low-tech cyclist
Don’t stop calling, this zombie is reanimated.
Alice Ollstein of TPM reports that Rand Paul will vote for the Motion to Proceed if guaranteed a vote on a clean-repeal amendment.
low-tech cyclist
@low-tech cyclist: Alice Ollstein of TPM reports… (just adding the link)
Arclite
What I’d really like to see is government sponsored regulation designed to reduce preventable disease. With so much disease caused by or exacerbated by obesity and diet, taxing things like sugar could go a long way in reducing consumption of unhealthy, disease-causing products (products, not food). It’s worked in both Mexico and Berkeley, so why not nationwide?
Since these diseases hit the poor in greater percentages, it’s a great way of reducing Medicaid spending without reducing Medicaid coverage.
Arclite
@Jeffro: The problem with such a high deductible is that people put of preventative care since they need it themselves. Then it becomes a 10-100x more expensive emergency. Ex: I had an infection in my thumb over the weekend, so I had to go to the ER. I will have to pay $100 for a $1000 ER visit. If I had to pay the full $1000, I would have waited. Dr. told me if I had waited another day, the infection would have spread to my hand, and I would have needed surgery: $10,000.
StringOnAStick
tRump administration MD’s like Price and those that agree with him are opposed at their very core to anything other than going back to the bad old days pre-ACA. Why? Because the only way this country is going to get to a Medicare for all or even Swiss style system is if downward pressure on costs happens, and that means putting the squeeze on providers like Price and his fellow dominantly reactionary orthopedic surgeons (you know, the guys who do a ton of joint replacements paid for by Medicare) plus every other high dollar specialty provider. I have to give props to the AMA for actually coming out against the BCRA, I figured they were still a bunch of docs with the same attitudes outlined above.
Becoming an MD in the US used to be a guaranteed ticket into the upper income bracket; now PCP and Internists are making about what a senior programmer makes while the expensive specialties like ortho surgeons, cardiologists, etc are still doing quite well but can see the writing on the wall: the way medicine is provided in the US has to either change or we accept that those without good employer provided health insurance are just going to have to do without and die. That’s it. Bringing down costs means some serious restructuring on how care is provided, from pharma to providers to everything in between. When an MRI in the US costs $1,000 and the same one is less than $300 in many European countries, something has to give.
I know some younger MD’s and they are much more likely to be supportive of the ACA since they’ve never been in the system when having an MD meant every patient you had paid out like a slot machine that’s always hot. These guys have seen the human damage that our crazed system puts the uninsured sick through and even that hoops the insured have to deal with. One is an anesthesiologist who is thrilled to work for an HMO because it means his hours are set and he can take vacations, something that is a big hassle in private practice. US patients want the same MD to see them, they don’t want who the pool sends when your doc is on vacation, whereas Canadians and Europeans are used to that system. I guess that means US patients don’t think their doctors ever need or should take a vacation, and for that these doctors think they need huge compensation (plus their medical school debt means they need it too). We have a friend who is a radiation oncologist in Canada, and who returned to Canada after growing heart sick about who got turned away from the CA practice he was in. He gets a decent but not enormous salary, nice vacation time, and 3 months of sabbatical every 5 years. I have often wondered if US docs would be interested in making that trade just for the reduction in stress and greater vacation time it offers, though maybe going to medical school in the US tends to self select for the hard driving and competitive individuals. My experience has been the older the doctor, the more opposed to the ACA or any change in how their profession is set up to work; and the opposite is true if the doctor is younger.
amygdala
@StringOnAStick: It’s not just age; it’s also specialty. A recent study indicated that surgeons, many surgical specialists, radiologists, and ED docs were more likely to be Republican. Probably not a coincidence that those are some of the most highly paid physicians. Gender probably also plays a role.
There’s a physician shortage looming, and burnout is widespread among health care workers, including doctors. It’s going to be interesting.