This is in response to a comment yesterday from Simon on my comment that the American medical system restricts doctor supply to increase incumbent incomes:
suppose you could build a medical system around undertrained practitioners who don’t even know what they don’t know, but why? Hating on doctors salaries and their “guild” is easy but analyzing how high their salaries really are when you take medical debt, hours worked and years of training into account is more difficult
Below is a graph of MCAT scores and science undergraduate GPAs of 1st year med school students by incoming class year from the Association of American Medical Colleges:
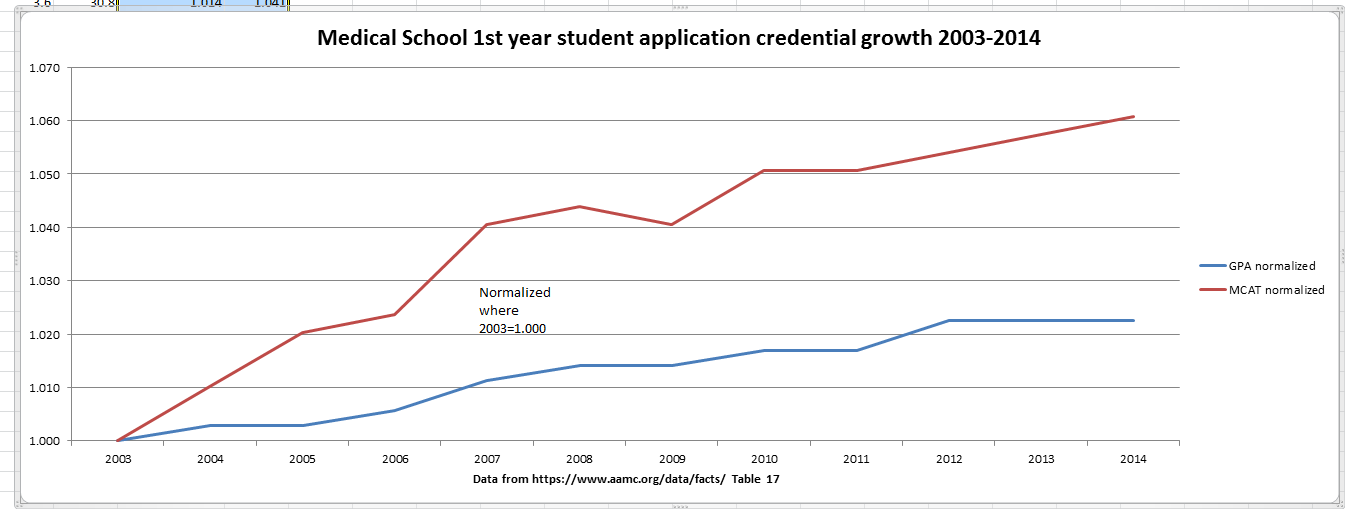
Is Simon saying the 2003 class of doctors (those are the docs who should be entering their prime earning and practice years right about now) are blundering idiots and that the only good docs are from the most recent classes as they have higher incoming credentials. Or have standards gone up (my quick back of the envelope story is that medicine is still extremely lucrative, and the bust of finance in 2008 plus the secular decline of the legal market is shifting some of the very smart people who aren’t quite sure what they want to do away from law and finance and towards medicine — one of my drinking buddies from college fits that description to a T) faster than enrollment capacity? If we as a society were completely happy with the doctors being produced from the 2003 first year cohort, what is the marginal gain in further heightening standards?
Are there people in the 2014 enrollment pool who have better pre-med credentials than below median 2003 enrollees who could not enroll?
Most likely yes, there are people in 2014 who were rejected everywhere who would have been accepted somewhere in 2003.
Are we better off with keeping those highly qualified people out of the medical training stream as they are no longer part of the potential guild, or is a slightly lower level of credentialing which allows them to do 80% as much as a MD/DO a good policy choice? Most people need primary care providers who can recognize common problems and also recognize things that look wierd and refer out. Would a person who was the marginal No for medical school in 2011, 2012, 2013, or 2014 be fully capable of performing that function, thus allowing a few more doctors to work higher up the care spectrum?
Cervantes
“Most people need primary care providers who can recognize common problems and also recognize things that look wierd and refer out. ” Those people don’t even need to be MDs. They can be NPs or PAs.
jake the antisoshul soshulist
I took him to mean Nurse Practitioners and Physicians’ Assistants. Who as we know are performing care that MDs once performed.
Betty
Do these numbers include the offshore medical students, of which there are many? With regard to Cervantes comment, I think that where the government could help in increasing the number of primary care physicians would be in assisting students with grants for their tuition in exchange for x number of years in primary care, especially in under served areas.
Richard Mayhew
@jake the antisoshul soshulist: Could be CRNPs, could be PAs, could be a a Jr. Doc or an Assistant Doc (I think a couple of Plains states are experimenting with that…) There is a large pool of very smart people who would have been med school eligible a decade ago who are still expressing med school interest but can’t get in … how do we use those people to perform highly needed and cost effective care?
Richard Mayhew
@Betty: The data set as I understand it contains all students who attend the first day of classes at a US med school, so yes, foreign students who are 1st years are included.
jake the antisoshul soshulist
I remember someone on C-Span suggesting that we address a shortage in GPs by subsidizing medical school for general practice.
JPL
@jake the antisoshul soshulist: Sounds like a great idea but you need schools to send them.
AMA is nothing more than a union trying to protect their own.
RSA
@jake the antisoshul soshulist:
I don’t know what drives med school costs, but that sounds good to me.
On the “[school] debt, hours worked and years of training” argument for high doctor salaries, I’d observe that lawyers are in the same boat, and no one wants to prop up their salaries. For what it’s worth, a lot of college professors are in that same boat, and don’t make half of what the average physician does.
Frankensteinbeck
Hey, Richard? I have a question. When I worked in a medical clinic, the constant refrain from the doctors was that the insurance companies forced them to go through extra, unnecessary steps – irrelevant blood tests, prescribing the wrong or a more expensive medication before they would pay for the drug the doctor thought was best. That kind of thing. How much is this a driver for health care costs? Is there any way, even, to measure it?
EDIT – @RSA:
Ballooning legal costs are not a major social issue. Ballooning education costs are, and in fact are complained about frequently and acknowledged as in desperate need of address.
Botsplainer
The bar to entry is needlessly high, the administration and faculty ridiculously overpaid. You could still lavishly compensate medical faculty at 1/3 current level.
Also, there needs to be room for no traditional students to enter – while I get the notion of requiring the lengthy education as a tool to get some “life-seasoning” into the mix so that empathy can be deployed, the system still devalues life experience by being weighted in favor of the young.
Further, there needs to be a great capacity expansion of med schools nationwide, classrooms to be staffed by interested retirees.
Callisto
It’s been a while since medical school, but I can attest to the change in attitudes in doctors just over the last 15 years or so (it’s been going on longer than that, but accelerating recently); it seems that fewer and fewer these days want to go into primary care/general practice. Everybody wants to specialize. NHS has been having a problem with this for years.
Suzanne
@RSA: Pretty much all the licensed professions are in that boat.
Tyro
Keep in mind also that the country produces roughly the same number of doctors when the country had 250 million people in it that is does when there are 300 million people in it. We have added about an additional country the size of France to our population, but did we add the same number of doctors that France has? No.
Plus, we have more intelligent people available to go into medicine but, once again, no additional spots in medical schools and residencies to absorb these additional people.
From my perspective in the tech industry, I would say that there is a large pool of very smart people in the tech industry who will eventually leave when they become disillusioned with the mediocre salaries and limited career lifespan who would have been happier in medicine (and in fact many will leave for med school).
Callisto
@jake the antisoshul soshulist:
Well, it isn’t just the fact that general practice isn’t ‘sexy’ enough for a lot of med students/graduates. GPs work just as many hours as specialists for what ends up often being less reimbursement, and huge amounts of time are spent on paperwork and bureaucratic stuff like fighting with insurance companies for authorization, disability paperwork, you name it.
Frankensteinbeck
@Callisto:
Oh, yeah. ‘If I were in it for the money, I’d have become a dermatologist.’ I heard that aaaaall the time.
Botsplainer
Kentucky governmental salaries.
Keep in mind that the coaches actually make a metric shitton of money for the schools from outside sources.
http://datacenter.courier-journal.com/government/salaries/
Callisto
@Frankensteinbeck:
Yes. Also, GPs have a role that other specialties don’t – in a functioning system, ignoring emergency care, a person’s PCP is their liaison to the medical/hospital establishment. He or she is the patient’s advocate. Some doctors find that job important and fulfilling, some don’t. Some start out feeling the former and burn out due to dealing with the insurance companies.
RSA
@Frankensteinbeck:
No disagreement here. The context for my comment was that high salaries aren’t a good solution for the high cost of education and other issues.
Amir Khalid
It’s a perennial problem with the medical profession everywhere in the world: the greatest need is for primary-care physicians, who see the most people, and see them the most often. But they’re the bottom of the doctors food chain; the professional prestige and the big bucks are in specialisation.
Wag
The biggest issue with expanding medical schools isn’t difficulty in expanind slots in the shcools, many medical schools (including my alma mater, Colorado), are doing exactly that. The difficulty comes with post-medical school training in Graduate Medical Education programs (ieinternship and residency). Finaincing GMEis very expensive, and is largely finaced through Medicare subsidies for patient care. CMS is currently rachting down on these payments, restricting the number of training slots available. Fro details please see this article from The new England Journal of Medicine http://www.nejm.org/doi/full/10.1056/NEJMp1306445?viewType=Print&viewClass=Print
Big ole hound
Most of the doctors I am forced to use or see around a hospital are from SE Asia, so how does this information apply to their ability? How does an MD degree from India or Pakistan compare to USA standards. The East Asian docs I have dealt with seem to have no idea about “quality of life” and my experiences have been very poor.
Tyro
@Amir Khalid: the professional prestige and the big bucks are in specialisation.
Yep. The money many specialists make rightfully belongs to the primary care docs, without whom he specialists would not have any patients in the first place.
Amir Khalid
@Big ole hound:
Don’t foreign doctors have to pass a test to get their licence to practise in the USA?
bloomingpol
If doctors should make large incomes because of the debt they incur, what about all those other people who have enormous student loans? If this is a problem that is making healthcare costs increase, why not make education costs a target for reform?
richard mayhew
@Frankensteinbeck: It is real, but I don’t know by how much
blueskies
@RSA:
Ahahahahah! Yes, that IS a true statement, just a little imprecise. If you change “half” to “a tenth,” you’d be heading in the right direction.
Callisto
@Amir Khalid:
Likewise being a GP isn’t really going to give you the chance to move up to the position of Chief of X at the hospital or Chair of the Department of Y at the university medical school. At least compared to everyone else.
Callisto
@Wag:
Internships are becoming a huge issue in all sorts of clinical areas. Ask a fourth- or fifth-year clinical psychology doctoral student how the internship situation is going these days.
Stella B
Richard is looking at a down period in the economy. When I went to medical school the economy was booming, nobody wanted to go to medical school and anybody, including me, could get in. Professional schools always have higher application rate during down turns in the economy.
Stella B
@RSA: Doctors in academia make less than doctors in private practice. PhDs in industry make more than PhDs in academia.
Callisto
@bloomingpol:
Medical school tuition isn’t as bad as most people assume, but combined with four years of undergrad at a decent school the debt load can be insane. It isn’t like grad school where your tuition is covered (or should be). So that’s eight some-odd years of loans unless you’re lucky enough to hook up with either a scholarship or at least an undergrad at a good but very cheap university.
Capri
@Frankensteinbeck:
Good luck with that – dermatology is by far the hardest residency to get into. Because the dollars earned per hours working is one of the best if not the best for all the specialties.
It’s interesting that despite being able to select the med. school students with the highest GPA and board scores, so little original research or advances are advanced by dermatologists.
There exist a fair number of small programs that pay debt or lower tuition for med students that go into under-served fields such as general practice, pediatrics, and psychiatry. My son looked into them when he started med school. Ultimately he decided not to apply for them despite wanting to be a pediatric psychiatrist (or join the Armed Forces, which is an excellent deal for med students) because the ones he looked into were oddly restrictive in too many ways.
Mnemosyne (iPad Mini)
@Big ole hound:
My current doctor went to medical school in India (in the 1970s) and is just as interested in holistic care as any US-trained doctor I’ve seen. I think it has a lot more to do with the attitude of the practice and what doctors they hire than where someone went to school.
a hip hop artist from Idaho (fka Bella Q)
@Callisto: That liaison role of primary care is sadly overlooked. With the administrative burden of insurance, it can no doubt be challenging to fulfill. Setting aside for the purpose of this comment the raw numbers shortage given population growth and geographical access issues, we don’t have a health care problem in the US so much as we have a health care payment problem.
Mnemosyne (iPad Mini)
@Capri:
Do you remember what some of the restrictions were? I think one that I heard of was that you had to both go into an underserved specialty AND agree to go to an underserved area. I could see doing something like a series of steps (you can get X tuition remission if you become a pediatrician, you can get X+Y if you also go to an underserved area, etc.) but making it too restrictive would seem to defeat the purpose.
Tripod
@Frankensteinbeck:
To be fair, a big part of that business is cash rather than insurance.
Frankensteinbeck
@Capri:
That is one disturbing, messed up job. Ugh. Desperately needed, but I wouldn’t want it.
richard mayhew
@Stella B: Look at 2003 compared to now.
I agree, the economy probably had a bit to do with the change as I noted:
Citizen_X
@RSA:
No to mention the visiting profs and adjuncts, who teach two thirds of all college classes, and all the researchers stuck in post-doc limbo.
In the case of the adjuncts, their “reward” drops all the way down to the poverty level.
Timurid
@Suzanne:
Yeah… when I looked at that graph the first thing I thought of was how the trend for academic employment looks just like this. They just do the big sort at the end of the training process instead of at the start.
JCT
@Callisto: Not to mention the fact that with the increase the % of women in med school (~25% back when I was a first year to 50% now), many med students are now marrying each other – doubling that debt. 400-500K for the both of them is not out of the question. Staggering when you are just getting started.
C.V. Danes
Seems to me that accurately describes the state of the medical profession for the entire history of the human race until about the last hundred years.
I would hazard that for the vast majority of ailments, a registered nurse could handle the job more than adequately. Indeed, I suggest that the problem with the current system is not adequate access to highly trained medical personnel, like doctors, but adequate access to medical personnel with any training at all.
Ask your average homeless person whether he would rather be seen by a doctor or a nurse, and I think he would just be happy to be seen by someone, period.
PurpleGirl
During college (1969–74) I hung out with Pre-Med Biology majors. I was the listener for several classes as they applied to med school and waited for the result. For most of these students, it was a harrowing period, fraught with fears and dreams. Even the students who had great grades and references — the brightest of the bright — approached applications with trepidation. It seemed to me that the med schools were contact with each other and each student was only going to get one acceptance. It can drive a person to depression when after making 10 applications, you get a few denials, then a few waiting lists and then the last school responds with the acceptance. And they not be the school you really wanted to go to, but it is the school you will go to.
ETA: I am convinced that schools and the medical guilds do restrict the number of people allowed in medical school to restrict the number of doctors in practice. With no regard to quality of the final product.
pseudonymous in nc
Actually, it’s pretty fucking easy: American doctors are mostly really rich. Even with a metric fucktonne of medical debt and years of training, they’re really rich: you don’t hear of that many doctors who are still paying more on their tuition loans than their mortgage in their late forties.
The American doctors who aren’t really rich are the ones that the US healthcare system needs. Fewer dermatologists, more general practitioners. Stuff their mouths with gold. And med school doesn’t need to be grad school: that’s a century-old relic.
Capri
@Mnemosyne (iPad Mini):
That is my recollection, too. It’s a given that you have to be practicing a type of medicine that is under manned. They you are sent to an under-served area. Once there you have to document that you are spending most of your working hours in that under-served area for several years. (That was the 1 hoop too many for my son). While it makes sense that you don’t want to send someone to Compton only to find out that they are spending 75% of their time at their Beverly Hills office (and no doubt folks did this, which is why they are making sure it doesn’t happen again), having to document how you spend your every working hour for 4 years is a big ask.
PurpleGirl
@Capri:
…having to document how you spend your every working hour for 4 years is a big ask.
Attorneys and their staff have to do this. Some firms want the diary in 15-minute segments, some want it in 10-minute segments. But for billing purposes, you have to note every client and every matter you worked on each (and every) day. I did it for the four years I worked as a paralegal. You get into a habit of noting times and issues you worked on. It’s doable.
ETA: Not keeping your diary or keeping it sloppily can get you fired.
Capri
@PurpleGirl: Yes, it can obviously be done and no doubt there are many medical students that are willing to do it or the program would have to alter its requirements.
If an organization had a goal of increasing the number of GPs, there are easier ways to do it than what is currently available.
Callisto
@Capri:
Not if it forgives a huge amount of debt. Paperwork sucks, but massive loans suck a lot more.
bornagaindem
Keep in mind that the AMA is the only system in the world where doctors have a graduate degree. In the rest of the world including Britain and Europe an MD is an undergraduate (albeit usually 5 or so years). Does the US have a better medical system than those countries? No. The AMA clearly wants to keep control of the supply of doctors in the US to keep salaries high. Instead we end up importing doctors from poor countries – how many of you live in rural areas where you can only see an Indian or Chinese doctor who does not speak great english (that is certainly the complaint of my in-laws in DuBois PA) That is because “real” doctors do not want those jobs – they are not lucrative enough. I for one would certainly like to see the strangle hold of the AMA broken and more medical schools or 6 years medical programs instituted. We are facing a doctor shortage that will be filled by immigrants instead of americans who with the proper education and access can fill those jobs easily. It is the same thing corporations have done with undermining the value of engineers- they can get cheaper ones from India and China because when your population is 1 to 2 billion that leaves a lot of smart people you can skim off of those societies. Then they try and convince us that we can’t produce enough educated people to fill the jobs they need when the only real problem is they can’t find americans stupid enough to do the job for the low salaries they want to pay. And year after year they get away with it.
Lurking Canadian
@PurpleGirl: The phenomenon is even more pronounced now. Basically every applicant to medical school aces the MCAT and graduates with perfect grades. I am convinced that they could accept twice, or even three times as many applicants without a dissolution of quality. They could pick at random from the top half of the applicant pool and get a perfectly acceptably crop of new doctors.
Instead they put the applicants through a bizarre ringer of interviews, mock patient interviews, role playing and butt kissing and THEN pick randomly.
RSA
@Citizen_X:
That’s the shame of U.S. higher education, I think.
mai naem mobile
You talk about physicians. Physical therapists are just as bad. The physical therapy boards and orgs.have been very successful at limiting the number of therapists in school here and the number coming in from other countries. I’m not so sure about occupational therapists but that may just be because the need for pts is much higher than ots. There’s not a whole lot of speech therapists out there either.
muddy
@Callisto: Indeed, you can work a minimum wage warehouse job and have to account for 10 minute increments of tasks over the workday, even though these are mixed together and sporadic over the course of a day (2 minutes here and there). There is even a special code for how long it took you to recover after a small injury, one that didn’t require medical attention. You need to account for the 10 minutes it took you to wash up and put a bandaid on.
Every month they come around and discuss with you what percentage of your time was in what category (down to 2 decimal places) and how you suck compared to the numerical standards they have set. They do not discuss your performance in terms of keeping up compared to your co-workers, it’s only in reference to their imaginary numbers.
This for minimum wage, I’d not have grumbled about it if I got tuition or something out of the deal. As it was, I grumbled.
Calouste
@bornagaindem: A lot of European countries have a numerus clausus for medical studies, because you can kind of predict based on population growth how many doctors you are going to need in the future, and you don’t really want to give these people a very expensive education, mostly paid for by the state, that they are not going to use.
But I’ve never understood why Americans need to faf around for four years in Biology or whatever before they can start in Medicine.
Capri
@Lurking Canadian:
Uh, not really. You can read lists of the cut-off GPA and MCAT scores for all the various medical schools in the country. For most, being essentially a B+ student is OK. It is harder to get into dental school or veterinary school than medical school- the barrier to entry to medical schools isn’t tremendously high actually.
Face to face interviews are a good way to identify the nut jobs and delusional and deny admittance rather than flunk out applicants that will not be successful.
And anyone who wants to be a physician but has poor grades can always go to one of the Island schools, whose entry requirements are much lower than the most lax American school.
bornagaindem
completely true and I agree but remember at least in england kids going to college have already specialized in their last two years of high school while in the US they are taking everything from english to PE even if they are going to go into the sciences. ^ year programs should be the norm here.
JoeShabadoo
@Capri: but anyone just can’t go and move to the islands while “paying” formedical school.