JAMA in 2016 published a great article that traced who received care and for what categories of need. **
I just love this visualization. I think this is my second favorite health policy visualization behind the bottom 50% of spenders drive 3% of costs curve.
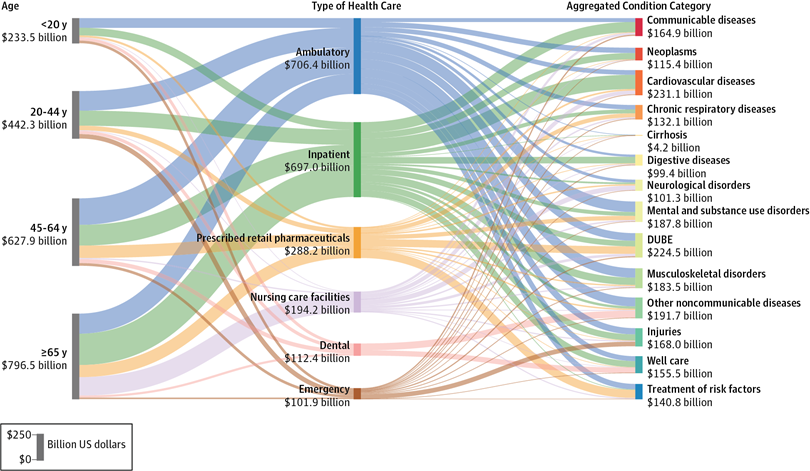
DUBE indicates diabetes, urogenital, blood, and endocrine diseases.
So what are the take-aways?
- Kids are cheap
- Medicaid and CHIP are decent safety nets for kids that need to improve but improvements are fairly low cost
- Emergency services aren’t that big of a slice of the pie
- Old people are expensive
- Medicare already acts as a quasi-high cost risk pool for the rest of the system
- Well care is fairly small
- The policy fight is really over 20-64 year olds
What are your take-aways from this image?
** Dieleman JL, Baral R, Birger M, et al. US Spending on Personal Health Care and Public Health, 1996-2013. JAMA. 2016;316(24):2627–2646. doi:10.1001/jama.2016.16885
batguano
Don’t get sick, but if you do die quickly
AnonPhenom
Who picked the breakdown on the right side of that thing? I’m clinically cringing here.
MomSense
@AnonPhenom:
Thank you. Aargh.
I guess it’s what is not on this chart that worries me. I think we should be spending a lot more on treatment of mental health and substance abuse because we certainly spend serious money on the related tragedies.
The other interesting thing is all the money spent on pharmaceuticals for managing chronic conditions. Some of that is just the volume but I wonder how much is because the pharmaceutical companies don’t invest in drugs for people with rare conditions. A friend of mine who went to the dark side and got a job with big pharma told me that they don’t invest in what they can’t market.
Another Scott
Your quote box spoiled my joke – “Why are DUBEs so expensive? Can’t people just grow their own these days?” ;-p
It would be interesting to see how this graph has changed over time, and how much of the cost are driven by more people getting care vs increased costs from expensive hardware, expensive medications, direct-to-consumer advertising, and salaries and stock options for executives, etc.
It would also be interesting to see how the costs have snowballed over time.
(I may have told this story before) – E.g. the friend of a friend who couldn’t afford dental work, got a bad abscess, got a blood infection, had his heart valve damaged, had surgery for the heart valve, “died on the table”, was revived, got addicted to opioids during recovery, had continuing issues, died in his 40s. All because of lack of appropriate dental care early enough. Because it’s “too expensive” for the USA to have decent low-cost dental services for everyone. :-(
Thanks.
Cheers,
Scott.
Pete Mack
Obesity is really expensive.
MomSense
@Another Scott:
I fucking hate this. We have one body. We’ve known for decades that oral health affects overall health. Also too good luck finding a job if your teeth are fucked.
Same for vision care. It’s obscene the way we treat health care in this country.
Barbara
My take away is that diabetes is going to bankrupt the system. Either that, or it will be found to be a significant cause in the plateau or even decline of life expectancy when they measure it in 2030. Yes, obesity is probably the underlying cause, but the diabetes pipeline is just getting started.
Cermet
Biggest take away? Easy! That Dental is grossly under funded (compared to real need) and would likely be larger than any single part on that display if it wasn’t.
Ceci n est pas mon nym
What’s the color coding on the bars on the far right? What does it mean for instance that Communicable Disease has a bright red bar and Injuries a sort of turquoise?
I love good visualization, and I love studying things like this for lessons. Going to take a while to digest.
One observation: I’m not surprised that the users of Nursing Care Facilities are overwhelmingly over 65. I am surprised that the Nursing Care beast has so many approximately-equal arms on the right, i.e. that the causes requiring residence in a nursing home seem to be pretty evenly spread across the spectrum.
ChicagoPat
How does this account for inpatient admissions that go through the ED? I’m an ER physician, and I can tell you the vast majority of the hospital admissions at *every* hospital I’ve worked at, come in through the ED. The fraction represented here as “Emergency Services” seems ludicrously low.
David Anderson
@MomSense: The failure of decent dental insurance is tomorrow’s post (and it is tied to the head/body split problem which leads to really strange market incentives)
David Anderson
@ChicagoPat: The sequence of initial appearance at the ER and then admission would be coded as an an Inpatient stay…
Litlebritdifrnt
I have told the story many times about I had a crown fall out in the US. I booked an appointment at the dentist to have it glued back in (there was nothing wrong with it, and the post was clean and still in place.) The dentist and his staff tutted and oh deared for 30 minutes while looking in my mouth and told me they would put temporary adhesive on it just for appearance sake but I would have to go back in two weeks to have x-rays, scans, full work up and gawd knows what else before they would even consider just reglueing the crown into my head. Cost? Between $1500 and $2500. I of course didn’t have the funds so I never went back and ended up using Fixodent every morning so I wasn’t walking around toothless. Until I went home for a visit. Went to a British dentist, lovely lady, gave me an examination, checked the crown and post, glued it in with permanent (extra strong) adhesive and job’s a good ‘un. Cost 80 quid. I told the dentist the story of my problems in the US and she said to me “they wouldn’t just glue it back in? What the bloody hell is wrong with that?” She explained that there was absolutely no reason for them not to glue the crown back in other than to make money off me. Story of my life in the US.
Barbara
@Ceci n est pas mon nym: It’s a little hard to compare, but it looks like cardiovascular and neurological (dementia) causes are the fattest lines in the nursing facility category, which would not be surprising.
Barbara
@Litlebritdifrnt: There is probably greater variability in the U.S. on things like this, but my dentist has glued crowns back in without insisting on a new one. Indeed, when I was resigned to getting a new one, they insisted on trying to preserve the old one.
Barbara
@ChicagoPat: It doesn’t. You would need an intermediate step that showed ED to Inpatient.
Ceci n est pas mon nym
@Litlebritdifrnt: I lost a filling in Denmark. It took them a while to figure out how to charge me, but they finally found a non-resident charge sheet and ended up charging me something like 2400 Kroner (about $300 I believe).
Two things I learned about Danish dentistry:
– apparently Danes aren’t into pain-killer. They were uncertain about even giving me any, a little surprised I asked for it, but when I told them I’d never had drilling without it, they agreed right away.
– whatever they use for pain killer in Denmark is strong stuff. I’m used to being able to function more or less normally 2-3 hours after the appointment, but they numbed an entire side of my face and it took me all day to get the feeling back.
Could be that #2 is related to #1, that having decided I was a wimpy non-stoic American, they gave me a bigger dose. Probably a Dane would have just been asked to bite down on a herring or something.
MomSense
@David Anderson:
Have there been any studies done (would it even be possible) to figure out what the financial costs of lack of dental and vision care are?
You’ve got kids who are really behind in school because they don’t have the glasses they need. You’ve got people who don’t find out they have macular degeneration, glaucoma, and other eye diseases until it’s too late.
When it comes to dental care, there are the deaths from abscesses and infections but there are also loss of income issues because people can’t find work when they are missing teeth or have diseased teeth, and there are nutritional consequences when people cannot chew fresh fruit and vegetables and other healthy foods.
David Anderson
@MomSense: It would be possible to get these studies done.
I am familiar with some studies that look at offering no cost sharing dental care to patients with cardiology issues as a net cost saver and health improver as dental care reduces inflammation which reduces high cost cardiac events.
I have never looked for dental/vision costs as a comprehensive analysis before.
catclub
after communicable diseases, neoplasms (cancer), come cardiovascular diseases, then respiratory diseases, then digestive diseases, cirrhosis, DUBE, then neurological, and musculoskeletal, What is left for ‘other non-communicable diseases’? Dental ( as others have mentioned)?
catclub
@Ceci n est pas mon nym:
This probably has its roots in the figure Tufte copied for ‘The visual display of quantitative information’ on Napoleon’s disatrous Russia Campaign.
The graphic shows about six dimensions of information, from time, to numbers of soldiers, to location, to weather ( I think).
gene108
It is confusing to follow. I think it is a bad graphic. Doesn’t communicate information easily.
*********************************************
On the contents…I don’t think it is between 20-64 year olds…I think it is between 40-64 year olds. After 40 is when all the partying you did earlier comes back to bite you, if you aren’t looking after your health. I’d say the difference between a normal 35 year old and a normal 20 year old is minimal, in terms of health care costs. 35 y.o.’s may not be young and invincible, in their minds, unlike a 20 year old, but unless they have some sort of genetic condition that requires regular treatment to manage (e.g. hereditary high cholesterol), the ills of modern society won’t manifest in most 35 year olds, so from a coverage standpoint they’d be about the same, in terms of usage of medical services.
The issue is what do you do, when people start aging into their 40’s and 50’s and how do you distribute those costs. To me, you spread the risk around the younger healthier population, but Republicans want to drive rifts between people, so they are trying to push young people onto cheap plans, because all many young folks think they need is “hit by a bus” coverage and concentrating the risk in older folks driving up their premiums. I guess the Republican goal is to get everyone so pissed off about healthcare, they give up on the idea of universal healthcare.
Anyway, the issue is how do you distribute the risk of chronic conditions that manifest in 40 and 50 year olds, so premiums don’t go crazy for some folks.
Barbara
@gene108: One of the most striking things to me is the prescription drug utilization data:
1. The amount for those who are 45-64 doesn’t seem all that different from those over 64. That is a statistic I find surprising, although maybe it’s more attributable to the fact that the 45-64 cohort traverses 20 years, and life expectancy at 65 still doesn’t reach an additional 20 years, especially for people taking a whole menu of prescription drugs. (That, all by itself, explains a lot about prescription drug marketing.)
2. After DUBE, the highest drug spend is for mental health and chronic respiratory conditions: Asthma and anti-depressant drugs.
somedoc
@Ceci n est pas mon nym: People rarely wind up needing long-term nursing home care for just one thing. Unless that thing is dementia, or maybe stroke. That’s why I’d guess the two thickest nursing home lines link to neurological and cardiovascular disease. Otherwise, and even often with those two, it’s the combination of many problems that leads to requiring nursing home care.
stinger
IANAD or N, so where on the right would gynecological and pregnancy care fall? Well care?
Feathers
1) The best dental plan I was ever on was one where the reimbursement rates for fixing things was based on how frequently you came in for cleanings. If you got your cleanings every six months, coverage for everything else was 100%, the rate dropped based on how up to date you were with basic care. I have terrible teeth, but this plan kept them in great shape.
2) The US really needs a nurse practitioner level of dentistry providers, who can handle cleanings and simple fillings, without direct supervision, passing more complicated procedures on to dentists.
3) We need a full medical model for obesity treatment and studies, that remove morality from the situation. We need to treat obesity studies like cancer ones, where all studies have to use the same rules and guidelines. Now, studies really massage the data, and thus give crap information. The data on obesity that comes sideways from cancer and psychiatric research gives different data from obesity studies.
Ab_Normal (at work)
A friend who is in her 30’s recently had all her teeth pulled (they were that jacked) but can’t yet afford dentures. Same friend has Hep C that they’re treating with “watchful waiting” because she can’t afford the treatment. Go go gadget US insurance system :(
David Anderson
@somedoc: I’m working on a hospice research project right now and usually by the time someone is hitting hospice, they have a primary diagnosis and then three to five other categories of comorbidities.
Quaker in a Basement
My takeaway? Someone has been studying Edward Tufte.
jl
Thanks for pointing out this article. Many good comments above.
My two cents. A lot of the data comes from the Medical Expenditure Panel Survey (MEPS), which systematically omits a lot of care incurred by anyone who is institutionalized in some sense. So, prisons, nursing home care, military utilization will tend to be under-estimated. Most good studies try to correct for that by adjusting estimate using other surveys that have better coverage. Maybe that is where the MarketScan data come in. Anyway, would have to get into the weeds on methods to see whether and how the authors adjusted for that. The MEPS bias on utilization cuts across age groups, so not sure how that affects overall spending by age, but the width of the costs due to various services may be affected, since there is a strong age profile there.
What strikes me most about the graph is the profile of total costs by age group. Looks like profile enforced by PPACA is about right, or if anything gives a little too much room for price discrimination by age, which is more about profits than cost of care. Really high age differentials in cost are more about what could be called gouging. It is like the gender differential. Over the liftespan, you might be able to justify charging women 5% to 10% more, since there is evidence that men are more expensive in some age groups (older adults, for example, when some men get weeded out due to younger heart attacks and strokes). But what happens when you allow insurance companies and providers to use price discrimination, and you don’t have lifelong policies (instead we have annual policy contracts) women get soaked and pay double or more, which is where the real trouble comes in. On balance, better to force risk pooling than allow gouging, since that, along with cherry picking, cream skimming and weeding out anyone who has slightest history of a problem, is what gradually destroys insurance markets in health care.
jl
Also, for those commenters interested in trends across time, some graphs showing trends are at the bottom of the JAMA article. Not sure whether it is behind a paywall for those who can’t get on internet through an academic connection.
StringOnAStick
@Feathers: 2)
Colorado has this, it’s called an Advanced Dental Hygiene Practitioner, but they are required to have indirect supervision by a dentist. The idea was to get cheaper providers into dentally underserved locations, towns too small and remote to support a dentist; success in recruiting students and getting them deployed to these areas has been mixed due to the expense of setting up a full office with X-ray facilities, sterilization costs, supplies, paying for supervision, and being in communities where people often can’t afford even lower cost care. What insurance will pay for cleanings and X-rays isn’t much more than the cost of providing those services and doesn’t do much to support any office’s bottom line; fillings and other dentist-provided care pays much better rates. The dental profession, especially corporate dentistry fought against allowing for advanced practitioners tooth and nail using the usual “not qualified, slippery slope” argument, and will try to kill it again in 7 years when the state Dental Practice Act is up for renewal by the state legislature again.
The dentists and especially the chain/corporate dentistry entities have much more lobbying dollars than the dental hygienists do, so for years there has been pressure to push as much of the “credentialed only” services as possible to dentists only, while cutting the dental hygienists into lower status and therefore lower salaries; the last thing they want is to allow advanced training to let a non-dentist do simple fillings. One state now doesn’t even require anything beyond a GED and training by a dentist to become what that state accepts as a dental hygienist (Alabama); the salaries there are less than half that of the national average (meaning no longer a middle class wage). So far the hygienists have held the line pretty well elsewhere, but the trend in dentistry is for large corporate owned practices, and that is sad in my POV because profit is the main motive. The days of the single or double dentist practice are drawing to a close, often because new dentists are getting out of school with so much debt (usually about $350,000) that they can’t buy into a practice so they end up working for the corporate practices where there are strong and consistent rumors of monthly quotas for procedures that must be met for financial incentives to accrue or to even keep your job; low producers get axed. You might have a tooth with a small cavity that gets upsold into full blown root canal therapy plus crown because someone needed to fill their monthly quota (saw this almost happen once, but fortunately the patient came to us for a second opinion).
Liltbritdifrnt’s experience is unfortunately becoming more common too. I temped as an RDH for 6 years and after working in perhaps 60 different offices I can tell you that there are always a few offices out there that look at each patient as a potential profit center first, patient second. Each profession has it’s professional magazines and there is a subset in dentistry that are all about increasing production (meaning profit) from each patient and how to make that happen. Here’s my list on how to avoid those places:
1) Ask a local you trust if they like their dentist and would recommend them; hell, ask several friends, then look the practice up on Google. Read the positive and negative reviews, and use a critical eye on the latter especially because even good offices get bad patients.
2) If FOX news is playing in the waiting room, leave, but first tell the receptionist why you are doing so. Have a good look at the magazines if you stay; Guns & Ammo is a bad sign. A large bible on display is also a bad sign.
3) If you get the song and dance that Litlbritdifrnt got about re-cementing a crown in place, say thanks, leave and get a second opinion.
4) NEVER go to an obvious chain with many locations in your city. Be aware of practices that have some location-based name instead of the dentist’s name(s); some of these are “hidden” chains. One I temped at had everyone on commission so of course it was in everyone’s interest to up-sell and up-diagnose as much as possible; these guys did it with a very heavy Christian prosperity gospel message to employees. Their RDH’s were making 40% more per hour than I do by making everyone a periodontal disease patient whether they were or not, but you can do that when you toss your professional ethics in the trash each morning.
5) If you feel like you are being sold on much more care and expense than comports with your prior experience as a dental patient, you probably are. Solution: second opinion.
6) Trust your instincts. Even if you have no dental background at all, if something feels wrong or aggressive to you, it very well might be. Again: second opinion.
7) You can look up a dentist’s name in the state licensing directory and see if there are any complaints against them from the past, what they were and how the dental board decided each case. If you see things like “sanctioned for false or misleading advertising” or “practice not meeting the current standard of care”, move on because this is a high pressure and/or low standards office.
somedoc
@David Anderson: Exciting research topic! “From the trenches”, hospice eligibility for non-cancer diagnoses often feels round-peg-square-hole. Especially for the very elderly. There is some clarity for a few specific conditions like ischemic heart failure and COPD. Dementia criteria are clear but overfitted to an unpredictable course. Everyone struggles with frailty or severe multimorbidity without a single obviously dominant fatal condition (the conditions are obvious, but which one will be fatal is not, and doesn’t even seem like the right question). Heck, often doctors struggle with what to list on death certificates for the very old.
Mnemosyne
@StringOnAStick:
Well, that’s horrifying. My (late) mom was a dental hygienist in the late 1960s/early 1970s and she was basically the dental equivalent of an RN. It sounds like states are totally degrading the title so that a dental assistant in one state can call themselves a dental hygienist in another. ?
Mnemosyne
@somedoc:
The top-line cause of death for my dad (at 74) was healthcare-related pneumonia, but the related causes were emphysema, kidney failure, and cancer (liver tumor and kidney tumor). Why, yes, he was a smoker, how could you tell? ?
StringOnAStick
@Mnemosyne: Well, it certainly depends on the state and Alabama is by far the worst in the country. The state that requires the highest standards and level of professionalism is California, which figures. Most states will accept a dental hygiene license from CA, CA is very picky which state licenses it accepts, and no one but Alabama accepts Alabama’s because it isn’t even a license there. The states least likely to allow dental hygienists to give anesthetic and in general to be seen as fellow professionals are mostly southern states.
The rules that cover dentistry and all the people working within that field are set by each state’s dental practice act; I know how it works in my state (7 year cycle for renewal of the legislation, which is when the window for change is open) and I suspect other states have variations on that. I think when Alabama fell into the current status for hygienists is about the time the national dental hygienist organization got a lot more organized so they could push back on such stuff, and so far no other state has gone the AL route. I don’t know any dentist who would want that kind of situation either, but I could see the corporate practices pushing for it because they could pay them less.
Personally it bothers we that there is such a wide range in quality of dental practice in general and dental hygiene practice in particular. Too many offices have their hygienists doing what can best be described as supervised neglect. Sure you’re getting your teeth cleaned every 6 months but maybe there isn’t much work being done below the gumline (which is where gum disease starts and hides) because they don’t want to use the ultrasonic scaler for some reason (usually the cost of replacement tips or the patient is too sensitive to it) or they don’t check the depths of the “turtleneck sweater” of gum tissue around each tooth at least once a year to catch this sort of thing before it gets past the point of being reversible. If you’re working for a dentist who doesn’t care much about gum disease then this stuff happens because if you’re the one crusading against it, the dentist will fire you as being “too aggressive” and the remaining staff will just keep toddling along. On the other side are offices that see the slightest bit of gingivitis and talk the patient into a thousand bucks worth of scaling and root planing, which is overkill for what needs to happen but is quite profitable for the practice. Unless you are in the field, you’d never know if you are getting good care or not. I had to force a friend of mine to quit going to a practice after I temped there because I wasn’t sure they were sterilizing any of the instruments to the current standards, and I definitely saw the dentist digging around in drawers of dental supplies with his spit covered gloves on (beyond gross, and so, so far below the legal definition of the “Standard of care”). They would go insane if I tried to take my used instruments into their sterilization area and would not let me enter that room, period, which made me very, very suspicious. Of course that dentist is a creepy all out tea party guy with his vehicle plastered with “those” bumper stickers, and stunningly greedy and a skinflint to his employees.
Mnemosyne
@StringOnAStick:
I have a very, very nice dentist who doesn’t have a hygienist anymore, just a dental assistant, probably because it’s a solo practice (though he did take on one additional dentist as a partner). He does my quarterly cleanings himself because I can’t tolerate the ultrasonic cleaner, and he does a deep clean with Novocain every couple of years (which is what my insurance company will pay for).
And he’s an immigrant himself (from Russia), so we feel comfortable talking shit about Trump while he works. ? Magazines are National Geographic and Better Homes & Gardens.
Ryan
Cirrohsis shows up on the chart, I guess because it’s a major cost. Yikes! Better cut back on the beer.
Barbara
@Ab_Normal (at work): Regarding Hep C drugs, I have read that insurers are trying in various ways to limit immediate access to the newer, much more expensive and much more effective drugs for people who have a recent history of IV drug abuse. They are scared to death that IV drug abusers being the way they are, the high rate of relapse means that Hep C will be a recurring problem. I don’t know what this means for your friend, but FWIW, she might be able to push a little harder. Also, there really are prescription drug assistance programs and your friend might be eligible for one.