I was planning on writing a 2,000 word response to an incredible article by Joshua Holland in the Nation. But I would get bored writing “ditto” too often. You should just read it. Here are some of the highlights of the pragmatic concerns about transitioning to a pure single payer system as the means to achieve universal or near universal coverage.
momentum is tempered by the fact that the activist left, which has a ton of energy at the moment, has for the most part failed to grapple with the difficulties of transitioning to a single-payer system. A common view is that since every other advanced country has a single-payer system, and the advantages of these schemes are pretty clear, the only real obstacles are a lack of imagination, or feckless Democrats and their donors. But the reality is more complicated.
For one thing, a near-consensus has developed around using Medicare to achieve single-payer health care, but Medicare isn’t a single-payer system in the sense that people usually think of it. This year, around a third of all enrollees purchased a private plan under the Medicare Advantage program….
fundamental problem is that compelling the entire population to move into Medicare, especially over a relatively short period of time, would invite a massive backlash.
The most important takeaway from recent efforts to reshape our health-care system is that “loss aversion” is probably the central force in health-care politics….
current Medicare-for-All proposals, we would be forcing over 70 percent of the adult population—including tens of millions of people who have decent coverage from their employer or their union, or the Veteran’s Administration, or the Federal Employees Health Benefits Program—to give up their current insurance for Medicare. Many employer-provided policies cover more than Medicare does, so a lot of people would objectively lose out in the deal.
Go read it. And then think long and hard.
Is your objective single payer as an end in and of itself? Or is your objective universal coverage as an end in and of itself with single payer as a potential means?
I am firmly on the universal coverage as the desired end in and of itself side of the argument. And that influenced how I read this piece as the pragmatic transition and loss aversion problems are real, they are are tremendously huge and they are tough problems to even frame much less solve.
Baud
Neoliberal.
bystander
Thinking is hard.
Sab
Mayhew Anderson: I read and really liked TR Reid’s book about healthcare around the world. I had no idea that there were so many options, and that insurance rather than single payer is the more common option.
Do you have an opinion about the accuracy and usefulness of this book as a sort of primer for those of us not down in the weeds trying to get an overview.
Formerly disgruntled in Oregon
Ditto
Baud
LGM had some excellent posts yesterday about health care and the ACA.
MomSense
The single payer advocates always say Medicare for all but why not Medicaid?
The other issue that has to be dealt with if we are ever to transition to single payer is medical school and specialists. Right now the whole system is geared towards maintaining a scarcity of specialists which keeps the costs up.
I personally prefer to see a nurse practitioner as my primary care provider but I don’t think there is widespread acceptance that we don’t need to have MDs do everything. Anyway, I just think that a discussion of how we train medical providers and who can then provide services has to be dealt with or single payer will always be too expensive.
Formerly disgruntled in Oregon
All change is resisted by most. Change that brings loss, doubly so.
David Anderson
@Formerly disgruntled in Oregon: Okay, so beyond a pithy saying, what is the plan to convert resistance centers into supporters or at least to bypass them?
Chyron HR
@MomSense:
Because Medicaid is insurance for THEM. Those people. Identity politicians. Schvartzers.
raven
@David Anderson: Tell it!
SFAW
A similar, but also interesting (to me, at least), graph might show what those percentages equate to in actual per capita dollars/Euros/lire/drachmas/RMB. (Maybe it’s in Holland’s article, but won’t get to read it until who-knows-when.) My interest is: how does our per capita OOP spending compare to the rest of the civilized world? (Probably should be normalized for median income, maybe that’s a separate chart.)
Naturally, if the USA’s OOP expense translates to $100 per person, that’s one thing. But if it looks more like $5000, then it’s an obvious problem. And if our per capita OOP is (let’s say) 20 times that of Canada, Germany, or the UK — or, perhaps, compared to a company with the same “healthiness profile” (meaning similar conditions/maladies are treated with similar outcomes) — then Congress’s brow might get even more furrowed.
Or, maybe, I have no fucking idea what I’m talking about. (Yeah, yeah, I know, Stop the Presses!)
ETA: The per capita OOP might be more useful as a median, not average, although “average” does have its value as well.
Another Scott
That’s an interesting graph. But I wonder if it is hiding more than it is illuminating. What is in the bin in “Out of Pocket” category in each country? Is it comparing apples to apples?
Would it make more sense to make it “per capita” rather than “per total domestic health spending”?
We know that the USA spends much more on health care than other modern economies (though by some measures the rest of the world is catching up, and the US rate of increase is slowing). But we also know that the USA often has worse outcomes (mother’s mortality after birth, infant mortality, lack of progress in life expectancy at birth for too many sub-groups, etc.). The “Out of Pocket” bin seems to be hiding something else important.
Thanks.
Cheers,
Scott.
SFAW
@David Anderson:
More Harry & Louise commercials?
JGabriel
David Anderson @ Top:
I think for a lot of people, the vagaries of the US gov’t (an increasingly right-wing GOP, increasing wealth inequality leading to increasing corporate power and influence, both major parties reliant on corporate donations, white majorities resentful of any aid helping minorities, etc.) indicate that any governmental system regulating insurance corporations will be subject to regulatory capture, deregulation, corruption, and dismantling any time a right-wing party takes control of the government – which we’ve watched the current right-wing gov’t attempt for the last 6 months.
That leads many of us to conclude that the best way to move forward is to eliminate – or severely curtail – corporate influence in US health markets, by advocating for some sort of single-payer system.
I agree that universal coverage, rather than single-payer, is the primary goal. That said, I’m not sure stable universal coverage is achievable, in the US, without implementing a single-payer system.
Sab
Why have my last two comments ended up in Moderation? They were beyond bland.
Never mind, One of them made out. Still bland, but there.
Barbara
OT: Can one of the FPs put up a post about the DC Meet up? My plan is to reserve a table at Elephant and Castle beginning at 5:15. E&C is on Pennsylvania Ave., NW between 12th and 13th Streets, across from the Old Post Office Building, now known as Trump Hotel. I will try to get there at around 5:15, and I will be wearing an orange dress. I would really like to know how many people (give or take) are planning to come so I get the right size table +2 (which I will just plan for). Thanks!
MomSense
@Chyron HR:
Pathetic but true.
gene108
From reading comments of liberals, single-payer is a means to usher in the glorious socialist revolution, wherein private for-profit businesses will be obsolete starting with private health insurance providers.
the Conster, la Citoyenne
@JGabriel:
As opposed to a governmental payer system? What about the Hyde Amendment? If the government pays, don’t they get to decide what’s covered? Look at the panel deciding women’s health care. Hard pass. It’s hard to imagine trusting insurance companies more than the government, but here we are.
Also, anecdotally, I hear that doctors are reluctant to take Medicare patients because reimbursements are so low. Along with single payer there would have to be a whole rethinking of doctor compensation, then medical school education costs, and then control over where doctors can practice, what they can practice, and how they can practice because of restraints on the kind of care that will be covered – especially end of life care. The bulk of Medicare expense for most people occur during that last year of life.
Barbara
@JGabriel: It depends on what people mean by single payer. Medicare is technically single payer (financed by government) but there are all kinds of private insurers that administer or implement or wrap around basic coverage. Medicaid is single payer within a state’s Medicaid population, but tends to rely increasingly on private insurers to administer benefits to certain but usually not all populations. So if the idea is to mirror that kind of system, my guess would be that insurers would figure out how to go along with it, but providers would go nuts, because it would effectively overturn the leverage they have built up in many places over payers. Providers have no pricing leverage with the state and federal government.
Kylroy
@the Conster, la Citoyenne: This. If your argument is that our government is prone to seizure by incompetent saboteurs at any moment, I don’t see how giving government *more* control over healthcare solves the problem.
And you point out that the big issue with implementing single payer won’t be fighting insurance companies – it will be fighting doctors. Not that taking on insurance companies is easy since they’re incredibly wealthy and connected…but doctors are wealthy, connected, *and* broadly liked by Americans.
gene108
@the Conster, la Citoyenne:
One thing that does not translate is when people say we should spend less on healthcare, someone working in healthcare will get less pay or money.
There will be a shock, if we suddenly switch to single payer.
We’ve already automated our way out of several career paths for people, over the last 40* years, which has forced people to look for work in other fields that pay well and are hiring. This leads a lot of folks into healthcare as medical billing specialists, for example.
* 40 years ago being a typist was a profession. We automated that need out of the workforce. Receptionists are not much needed anymore because phone systems are automated. There’s been job loss due to automation in fields other than manufacturing and coal mining, though those get the headlines.
gvg
I do of course want everyone covered.
I want it not possible for Nuts in elected office to hold it hostage at a later date.
End results like life expectancy and quality of life are the point.
I don’t want elderly people with senility setting in nor random people who were never that bright or even random people who have an average education that wasn’t in human biology nor insurance finance to be able to get care without learning the system. We all have our responsibilities, to ourselves, family, jobs and citizenship where we have to learn a system. we mostly cannot become a professional and the choices are just too overwhelming. I think this is behind the love for single payer. 1 system. simple. you get sick, you get the care. Thats what people want. If you are in pain, your mind does not work as well. If you are unconscious or under anesthesia your mind isn’t working at all. You can’t call around for instructions and a better deal.
I also think even the unemployed should be covered. That is not something conservatives or some liberals really believe.
don’t know how we get there.
tobie
Thanks so much for this post and the link to Holland’s article. I feel like the left has forgotten how successful the “Bismarck Plan,” as opposed to single payer, is in Germany and Switzerland. Both countries achieve universal coverage, and you can buy insurance on an individual market, though most people get their health insurance through their employer. It seems to make sense to follow this model if we don’t want to disrupt the economy by overturning the entire healthcare system overnight.
David Anderson/Richard Mayhew: I for one would be really grateful for an in-depth explanation of how the Swiss and German healthcare systems work. No pressure…but it would be nice if you had time and the inclination!
Ten Bears
It’s too hard, there”s no point in even trying.
Chyron HR
@JGabriel:
This is the absolute 100% best argument AGAINST single-payer (or any form of social progress based on government-run programs). America needs a form of universal health care that won’t get scuttled 4-12 years later when Republicans take control of the government again.
Kylroy
@gene108: I sometimes think that the wildly inefficient American healthcare sector has functioned as an accidental jobs program.
Villago Delenda Est
Who knew that all this could be so complicated?
I’m with David…I want universal coverage which means universal care. A system that removes barriers from basic care that can prevent complications and more expensive care down the road. This is how the VA functions…and it makes sense to me.
Ocotillo
@MomSense:
I believe doctors are reimbursed less for Medicaid so they would push back.
Villago Delenda Est
@gene108:
Well, we can start with CEOs of health insurance outfits, who like many CEOs, are compensated far in excess of any reasonable compensation.
sharl
@David Anderson:
I’m sure there are conventional – and politically influential – business and medical interests who would need to be considered in any proposed changes that might affects those groups’ interests.
I follow young lefties on twitter, a highly energetic but impatient and often frustrated/angry lot (that often comes with the youth thing, of course). When I read your post I immediately went to see the twitter feed of one of the popular young activists* on this topic (*he’s not really an expert in any classic sense; largely self-taught with some help from friends). He is an advocate for universal single payer (USP), and his response to Joshua Holland’s article is kinda what I figured it might be:
So there’s another center of opposition. I suspect a lot of the younger folk can be convinced – eventually – but it won’t be an easy sell. Tim Faust has something of a natural skill for winning folks over – he’d be a great televangelist if he had chosen to go that way – and his podcasts appearances are very enthusiastically received. And if I read his twitter feed correctly, he scored a meeting with @IronStache, a populist seeking to win the Democratic primary to challenge Paul Ryan in WI-01. So he gets folks to listen to him.
Many necessary discussions/arguments will be needed on this topic, I’m guessing, and it will be more of a marathon than a sprint. The old sports phrase “winning ugly” might best describe the most optimistic outcome IMO.
Rob in CT
David,
I’ve been meaning to ask you, have you seen this attempt to sketch out a single-payer proposal:
I saw it because Loomis over at LGM posted about it. I’d curious to see your thoughts on it.
the Conster, la Citoyenne
The idiot left also doesn’t seem to realize that there are more states in this country than there are countries in Europe, each with their own chief executive and legislature. The ACA was designed to get us most of the way to UHC, but red state governors petitioned SCOTUS and won to opt out of Medicaid – the government paid for health insurance for the poorest population – because it would help “those people”. Dear leftist idiots – please explain to me like I’m five years old how you sell single payer to white people – like the ones who voted for a governor in Kentucky who promised to take their own health care away – because it created a culture of dependency, if you know what that means and I think you do.
sherparick
@Baud: Yea. The purity trolls and Bernie Bros will just erupt on this one. By the way, although Senator Sanders really does attract some douche bag supporters, he himself has been stalwart in defending the ACA the last six months, and recognizing what a progressive law it is. As Scott Lemieux points out, Republicans and Conservatives hate this law with a passion because it is progressive and does so much good for so many people. http://www.lawyersgunsmoneyblog.com/2017/08/aca-consists-things-national-republicans-always-hated
This is what the ACA did.
The ACA essentially consisted of:
A historic expansion of the public insurance program for the poor
Increased taxes on the wealthy
Substantially increased regulation of the insurance industry
Subsidies to allow the non-affluent to purchase comprehensive insurance
And Republicans and the business elite hate all these things. And it literally drives them crazy, hence Trump is our President and we are all screwed. But besides the ACA and Medicaid, they also hate Medicare and Social Security and want to get rid of them (which is really the point of the Balance Budget Amendment and ALEC’s call for a rewrite of the Constitution, – they want Constitutionally abolish Medicare and Social Security and do it in a back door way). Until the Republican Party because a real, sane, Conservative pro-business party again, instead of being the Hell Spawn of a union of Billionaire Ideologues worshipping Any Rand, Christian Theocons dreaming to recreate John Calvin’s Puritan Dictatorship in the United States, and White Supremacists dreaming of a purging the country of all darker skin people that it is today, we will have to be ready to resist them at every election.
Despite all the clownishness and fail, on Environmental, immigration, and civil rights issues, the Trumpkins make things worse every day, one small change in Government policy and budget cut at a time.
NobodySpecial
One place that I think we can start to fix provider rates is by the government underwriting med school costs in exchange for at least five years after graduation as a GP. Hold the note in escrow while they’re practicing, and if they go five, tear up the note. Hell of an inducement to lower costs, I’d think.
the Conster, la Citoyenne
@sherparick:
The low info left don’t know how anything works, so they call everything neoliberal.
RobertDSC-iPhone 6
Federalizing Medicaid would be good. Remove the idea that states will do their own thing for their own people. Clearly this is not the case with states that did not accept the Expansion as part of ACA.
Rob in CT
edit: oops, duplicate.
Iowa Old Lady
@Ocotillo: They’re reimbursed less by Medicare too, which is why some practitioners take no or only a limited number of Medicare patients.
Also, I suspect many people don’t know that retired people often pay a monthly premium for Medicare, depending on their income. It’s withheld directly from your Social Security check.
Jim, Foolish Literalist
true, he has, after spending a few weeks telling his supporters that everything the Democratic party has done over the last twenty-five years has been a “fail-yuh”. Articles I read about the emerging strength of the left and the new litmus tests and how Kamala Harris is already a sell-out tend to feature quotes from the brilliant Roseann DeMoro, who I believe is a regular in his traveling show.
Rob in CT
@Jim, Foolish Literalist:
DeMoro is delusional. The one thing she gets right is that he’s “not about either party; he’s about something very different.” Yeah, himself. That’s it. There is no more.
the Conster, la Citoyenne
@RobertDSC-iPhone 6:
This is a great suggestion, but who would be voting on such a thing? It isn’t even thinkable until Dems get all three branches of government back with a mandate like LBJ had. The white nativists have captured the GOP, and no big government programs will ever be enacted until they’re sent back into their holes.
MomSense
@Ocotillo:
And this is why we need to deal with the cost of training people to be doctors.
the Conster, la Citoyenne
@Rob in CT:
I will never forgive that unaccomplished fucking fraud for conning a bunch of low info kids into thinking he’s the answer to anything.
Erin in Flagstaff
Kevin Drum had a good look at how one country got to single payer. It didn’t happen immediately: http://www.motherjones.com/kevin-drum/2017/08/single-payer-take-a-look-at-how-south-korea-did-it/.
He even tries to get a way we can get there with several steps.
Procopius
How about we just start by enrolling people in Medicare automatically when they start drawing their old age benefit? Lots of people have to do that at or shortly after age 62, but they can’t enroll in Medicare until they’re 65. Then let’s start looking at what it would cost to allow people to buy in to Medicaid coverage. I hate means testing, but their premium could be determined by some formula based on last year’s adjusted gross income or something. Something easy to prove, that’s already in the IRS data banks. Simplify, simplify, simplify. Make it easy. No upper limit. If some snollygoster making $25 million wants to buy in, let him. Just like I believe tuition at state universities should be free for every applicant, regardless of their parents’ income. It’s too costly and complicated to exclude people because they’re too rich.
the Conster, la Citoyenne
@Erin in Flagstaff:
South Korea is the size of Kentucky. Any comparison to other countries that doesn’t discuss how to get the red state Confederacy on board is useless.
Sab
Jackels got here, Why do I bother to even read or comment. Lots of political tirades.
No useful ruminating for those of us with skin in the game who don’t want our kids or grandkids to die of curable conditions. Lots of solutions, but the politically minded would rather rant about the other side than find solutions.
I agree the other side is worse than us. I don’t care. I just want my autistic, adorable three year old granddaughter to covered by medicaid.
Rob in CT
@the Conster, la Citoyenne:
I’ll never forgive the people who should have, and on some level DID, know better but voted for him anyway. I mean, I’ll pretend to forgive them, or try at least. But not in my heart. 63 million Americans utterly disgraced themselves and the Republic on election day last year. Millions more, actually, when you include the Stein & Johnson voters. And the people who went “eh, can’t be arsed.” A know-nothing conman is on the ballot, campaigning on hate and you can’t be bothered to show up? Citizenship failure.
Rob in CT
@Sab:
What does this even mean? I’ve read it twice and I don’t know what you want (from commenters here, about whom you are complaining).
Finding solutions = defeating Republicans, taking power, and using it to pass laws that provide universal coverage (and lower cost of care). If you still think there is some path forward that involves meeting the GOP partway, I don’t even know what to say to you.
Procopius
@MomSense: Yes. Medicaid would be a better option than Medicare. Also, the people buying in would be seen as paying, much like paying private health insurance policies. That should make it more politically palatable, and keep the tax burden down. Do away with the awful idea in ACA of making people predict what their income is going to be in the coming year. Lots of people don’t have any way of knowing. Use something like the adjusted gross income from their last year’s tax return. That’s already in the IRS computer system. If they didn’t file a tax return just take their word for what their income was. Means testing is a chump’s game. It always costs more than it saves. If they had taxable income and didn’t file, the IRS will get them eventually. They audit poor people a lot more than rich people. It would help if Congress would increase funding for IRS enforcement, too, but even Democrats don’t want to do that. It would be very much like the Public Option that was pushed off the table during ACA negotiations.
the Conster, la Citoyenne
@Sab:
We all have skin in the game. What are you talking about?
the Conster, la Citoyenne
@Procopius:
Joe Lieberman pushed the public option off the table. Another fucking preening asshole party of one Independent Joe Lieberman. Don’t ever forget that.
the Conster, la Citoyenne
@the Conster, la Citoyenne:
The way to get the Confederacy on board for single payer is the same way that FDR got Social Security and Medicare passed – by selling out blacks and women to second class citizenship. Everything is about race in this country, and has been since the beginning.
Jim, Foolish Literalist
I like the article, but this part early on bothered me a bit
Further on in the article he makes clear distinctions between “universal” and “single-payer”, but I wish he had done so in this paragraph, just for clarity. Some of the most passionate (loudest) voices on this issue conflate the two, and we get loud declarations that anything less than Single Payer is worse than the status quo, or the pre-ACA landscape.
MomSense
@Procopius:
We do currently use our adjusted gross incomes from our tax returns on the exchange. And then if something changes, like you lose your job or change jobs, that is a qualifying event that allows you to change your premium amount and/or plan through the exchange.
David Anderson
@Rob in CT: Yes, and I will have a longer comment this weekend after the wife and kids leave early to see the grandparents and cousins (I will join in mid-week)
Bob Collins
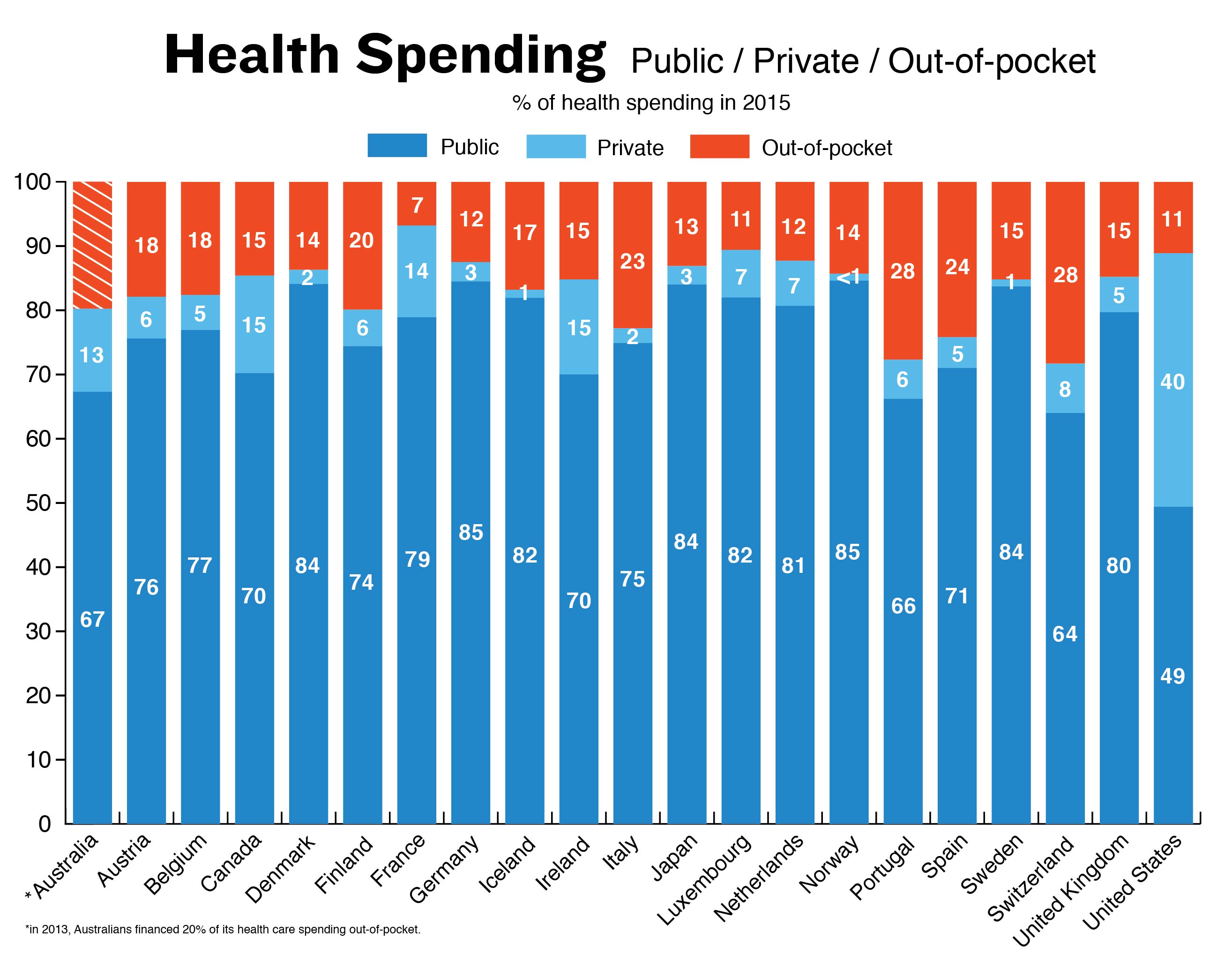
The graph is simply misleading. If the columns reflected actual costs instead of percentages of the cost, then one could see that the public part of US health costs is probably larger than every other country’s total health cost, except for Switzerland. Then one can make a straightforward comparison whether a public single payer is indeed theoretically feasible in the US, because we already have a single payer providing as much funding for health care as other countries.
Graphing actual costs instead of percentages of total costs would also show where the waste in this country is: with insurance companies, very high specialist salaries, and with excessive profits for private hospitals, medical device makers, and pharmaceutical companies.
Moreover, as mentioned above, how are out-of-pocket costs paid for in other countries. Are they subsidized for poorer citizens? Also, in a country like the UK where citizens and doctors can make private arrangements outside the national system, are those costs included in the graph? If so, should they be?
Single payer ought to be the goal, for it probably provides the cheapest way to universal coverage. Single payer all at once can’t be done, but we can start the process of whittling salaries and profits and relegating insurance companies to concierge-style medical care.
Miss Bianca
I’m so glad you cited this article, David – I just read it yesterday, and I’ve been trying to tell all my “single payer now!!” friends to read it, too. But since they don’t even want to acknowledge that single-payer and universal health coverage are not, actually, the same thing, and honestly/earnestly tell me that “the important thing is to pass the legislation and then work out the details” (gee, because that always works out SO WELL, amirite?), and then approvingly quote morons who want to make sure that Democrats tie themselves to this single-payer anchor OR ELSE, I…just don’t know. Honest to Dog, I thought leftists were smarter than conservatives, but it turns out that on certain issues they are just as unreflective and intellectually incurious.
BTW, did you read the coments on that article, and if so, did you think any of them had valid points in their criticisms?
azlib
One other problem getting to a single-payer system is where does the money employers save on health insurance go? If my taxes go up to pay for single payer, I am fine with that as long as the corporate expense for health insurance comes back into my pocket. If it goes to the stockholders I am not okay with that.
The bottom line here and as pointed out in the article, you simply cannot blow up a sixth of the economy overnight and not expect massive disruption and political blowback.
ThresherK
@Miss Bianca: I saw Dunkirk with two SinglePayerNow friends.
They kept asking me “Why aren’t the Allies marching on Berlin yet?”
LaNonna
Long time dual citizen resident of Italy lurkers here. The OOP expenses here are quite reasonable, and only apply to expensive specialist visits or tests (expensive, being about 30 eu). Any household of 4 with less than 24,000 eu per year in earnings gets a waiver on these costs (free) and pharmaceutical assistance, i.e., most repeat prescriptions for chronic conditions = 1 eu per 30 days. Also, mostly subsidised preventive care for the elderly over 65 and children under 6 (free), and your doctor visits are free. The family doctor is the lynchpin of care, educated by the state, a state employee, paid by the state, with state mandated hours and limits to # of patients in the practice. If you do not want to wait for a specialist appt, you can pay privately, about 100 eu, for the specialist visit, and take results back into the state system for continued treatment. Works really well, IMO
rikyrah
Thank you Mayhew
Rob in CT
@David Anderson: Woohoo!
Another Scott
@Bob Collins: Well said.
Cheers,
Scott.
StringOnAStick
Just after the Women’s March I went to a once a month group that had formed in this area, not an OFA or anything else affiliated, just concerned liberals (which around here means young white suburban moms). It had far too much of an “encounter group” feel to it and I soon realized it was a waste of my time, but there was a lot of Single Payer NOW sentiments expressed. I stood up and pointed out that there are other models, such as the Swiss model where there are insurance companies but they are heavily regulated and the end result was Universal Care. The look of shock that such a thing exists was nearly universal in that crowd, and it made me realize that a lot of the people getting “activated” as it were, are passionate but pretty uninformed. There was also an email from the group leader this morning that the group was no longer going have regular monthly meetings, just get togethers with the interested parties, which I think means it is back to being mostly the local concerned moms group and will be folded into the book club and babysitting coop (at least that \’s the vibe I got).
Miss Bianca
@StringOnAStick: Encounter group! Oh, yeah, the looks of shock when you tell people that there are *functioning* universal care systems that *aren’t* single-payer would be priceless if they weren’t so infuriating. But then, maybe I shouldn’t get so mad at people – my ignorance on the subject would be pretty vast if it weren’t for BJ and David Richard Anderson-Mayhew taking it on himself to educate a pack of snarling jackals. And even tho’ I knew it was mostly based on hand-waving and BS, I voted for the Colorado sinlge-payer initiative, so what does that make me?
David Anderson
@Miss Bianca: A lot of teeth were gnashed in the Nation comment section. A lot of handwaving going on about the difficulty of taking hundreds of thousands of dollars out of the pockets of the most trusted and liked people in America and a conviction that all of the waste is in the insurance industry or the C-level of the hospital and drug industry.
Eric U.
the potential backlash from the proposed California plan scared the hell out of me. I think if they implemented it, the republicans would have a similar advantage there to what the Democrats have now. ACA with a Medicare option seems like it would be the best way to go. The real weakness in the ACA is right at the lower end of the working class, where a lot of people have trouble affording insurance.
Miss Bianca
@David Anderson: That was kind of my impression as well, just wondered if you saw anything valid in the “but wait, you’re doing single-payer criticism WRONG and here’s why” stuff. You being the expert and all. ; )
BTW, sincere and multiple thank-yous for all the work you’ve put into turning me, among other jackals here, into a thorn into the side of my progressive betters. Still have a lot to learn before an airtight elevator speech about “this is why actually FIXING the ACA is a better bet than pushing for single-payer” can come springing from my lips, but I’m a lot closer to it now than I was a year ago.
p.a.
Way late to this discussion, just spitballing here, not worrying about $ just looking at getting people covered: newborns get insurance-for-life (levels, coverage t.b.d), everyone else, signup is voluntary.
They phased in Social Sec, correct? What about Medicare?
David Anderson
@p.a.: makes enough sense
Raven Onthill
I would say that an appropriate goal is universal non-profit coverage. That’s important, because the US system is dominated by rent-seeking behavior, making it extraordinarily expensive and inefficient. Now, this doesn’t mean that individual participants in the system can’t make a profit. It does mean that the overall operation of the system ought not be twisted out of shape by the goal of making as big a profit as possible.
NR
You guys are all correct of course. The only sensible course of action for our health care system is to continue allowing 20% of our health care dollars to go to insurance company profits. Anything else is just stupid and unrealistic. I’m sure glad we have you sensible centrists to tell us dumb liberals how the world really works.
NR
@ThresherK: I saw Dunkirk with a couple of my sensible centrist friends.
They kept asking me “Why are they trying to evacuate all the soldiers?”
jl
Pretty good article. Too much of it was spent bashing the simple slogans ‘single payer’ and ‘Medicare for All’.and all simple slogans, and then strangely in the middle suggests another simple slogan ‘health care is a right’ in their place. That, like other slogans doesn’t mean much. No right is unconditional, even more fundamental rights like right to free speech.
As an economist, I’d prefer that the ‘rights’ part be partnered up with the ‘how to pay for it part’. Maybe that is too wonky, but I’d try for the slogan Stiglitz uses, which is that in some types of markets, especially where different players have different sets of information, efficiency and equity are not opposing principles. Often the more equitable (‘fairer’) system is more efficient. I admit that slogan needs work.
I have some quibbles with the stats. The chart, which the author implies comes from OECD data, shows public insurance share that seems far too high for some countries. I wonder if the author misinterpreted the statistics and some of the private non-profit insurance is mistakenly categorized as public. Also, it is NOT true that all the of other, better, universal care systems were in place soon after WWII. Some of the currently successful systems, or systems that made big improvements (Australia, Switzerland, and Portugal) were developed from the mid-1970s through the late 1980s and early 1990s.
The article dances around the problem of oligopolistic local market pricing power of providers, and lack of price transparency in services, devices, supplies and drugs, pretty much everything, in the US. I also think it is over broad to say that all other countries with good systems handle the provider pricing power issue with ‘controls’. I’m not sure what the author meant by that term, but certainly not all countries control expenses by imposing hard price controls.
Applejinx
@jl: “in some types of markets, especially where different players have different sets of information, efficiency and equity are not opposing principles, often the more equitable (‘fairer’) system is more efficient NOW!”
There, fixed it for ya :)
These threads depress me for the following reason: the argument “gutting the insurance/medical sector to kill their profit taking will kill the economy” is TRUE. Yes, a lot of the culprits are wealthy and don’t spend money in the economy as efficiently as poor people do, but I know a LOT of people working in healthcare. You think the loss of long distance truckers will hurt the economy? That’s nothing to what an abrupt switch to an efficient non-wasteful single payer system would do.
But what people refuse to see is: continuing the profit taking will not help. There’s nothing healthy about the situation. It’s not heading anywhere good. And we’ll pay for having the culture that has set this system in place.
Preserving the rich doctors and all the countless white-collar health care workers in medicine and pharma will not save us. In that light, we might as well flip the switch now, because the consequences of lancing this boil are only getting worse as time goes on. We can process the obliterating of the for-profit healthcare sector now, or we can process it while also processing the obliterating of long-haul truckers, but all of this is going to go away.
Bleak, I know.
mere mortal
Reduce the age for Medicare coverage by one year every year.
It’s the easiest thing in the world. Slowly pushes inefficient insurance companies out of the market, takes on the citizens insurance companies least want to cover first, minimizes pressure on the Medicare program by not taking on the entire population at once.
Uncle Ebeneezer
@StringOnAStick: “Encounter group” Ha!! Welcome to every one of my Indivisible meetings.