When should people get treatment? Should people get treated for something as early as possible? Or should they wait until later when discrete milestones are passed? What does the decision tree look like?
The Incidental Economist passes along the latest research on the prostate cancer treatment debate. The United States has a culture of treatment as soon as prostate cancer is bio-chemically detectable. Most of Europe has a culture of treatment at a milestone.
NEJM, Anna Bill-Axelson and colleagues published the latest findings from the Scandinavian Prostate Cancer Group Study Number 4 (SPCG-4).
RESULTS: During 23.2 years of follow-up, 200 of 347 men in the surgery group and 247 of the 348 men in the watchful-waiting group died. Of the deaths, 63 in the surgery group and 99 in the watchful-waiting group were due to prostate cancer; the relative risk was 0.56 (95% confidence interval [CI], 0.41 to 0.77; P=0.001), and the absolute difference was 11.0 percentage points (95% CI, 4.5 to 17.5)….
Aggressive treatment works in this care. However IE also passes along a critique of translating this research into the United States.
Second, the results of this study aren’t necessarily generalizable to a US population, as Richard Hoffman explained.
PSA screening became widespread in the US in the early 1990s—a decade before the first SPCG-4 publication. Perversely, the American way was to expend considerable resources to promote screening efforts to find cancers…before knowing whether these cancers could be successfully treated. [So,] the SPCG-4 results are not readily translatable to US practice. Only 5% of the study cohort had cancers detected by screening PSA—the rest either had symptoms and/or a palpable tumor. In the US, a substantial proportion of men with PSA-detected cancers have microscopic disease—which may never cause problems during a man’s lifetime. The US Prostate Cancer Versus Observation Trial (PIVOT) also evaluated surgery vs. watchful waiting. However, PIVOT, which mostly enrolled men with PSA-detected cancers, found no benefit for surgery. Post-hoc analyses suggested that only the small proportion of men with higher-risk cancers (based on PSA and the microscopic appearance of the cancer) seemed to have a survival benefit.
The US research has found that aggressive treatment of bio-chemically detected prostate cancer does not do much to improve outcomes for the general population of biochemically detected prostate cancer patients. Aggressive treatment tends to have significant side-effects as well.
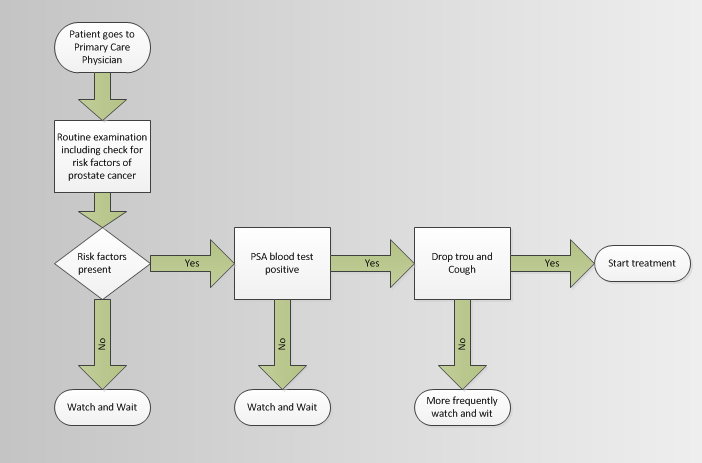
What could a potential decision tree look like that minimizes overtreatment while also minimizing undertreatment?