
We all want to talk about the distinction between light and not light treason… Or more realistically Espionage Act versus campaign finance violations.
Open thread.
![]()
Come for the politics, stay for the snark.
I am a student in the doctoral program at the Duke University Department of Population Health Sciences. I am working towards my my doctorate in Health Services Research with a policy focus. I am fundamentally fascinated by insurance markets, consumer choice and the navigation of complex choice environments. I'm currently RA-ing at the Duke Margolis Center for Health Policy.
I used to be Richard Mayhew, a mid-level bureaucrat at UPMC Health Plan. I started writing here and have not found a reason to stop.
Conflicts of interest: Previously employed at UPMC Health Plan until 12/31/16. I also worked full time as a research associate at the Duke University Margolis Center for Health Policy. I have received direct funding from the National Institute for Healthcare Management, and I have been on projects funded by the Rockefeller Foundation, Kate B. Reynolds Charitable Trust, Gordan and Betty Moore Foundation, Duke University Health System, CMMI, and various value based payment consortiums. I serve as a consultant on a grant from the Commonwealth Fund and have acted as a consultant to several ACA insurers.
Research Production is here: https://scholar.google.com/citations?user=zof9b4IAAAAJ&hl=en
David Anderson has been a Balloon Juice writer since 2013.
We all want to talk about the distinction between light and not light treason… Or more realistically Espionage Act versus campaign finance violations.
Open thread.
I just can’t figure out what is out there that makes releasing this tweet a good idea. Read about 3/4ths of the way down:
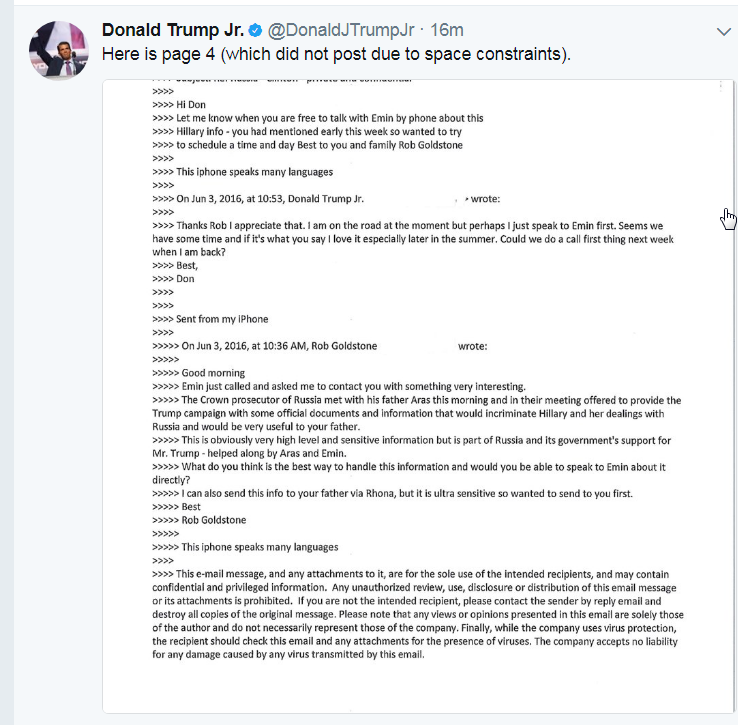
Update 1: A respected NatSec attorney’s reaction:
I literally do not understand what the hell @DonaldJTrumpJr is doing right now. This is simply too stupid to fathom.
— Bradley P. Moss, Esq (@BradMossEsq) July 11, 2017
There is a really nice little paper in this week’s JAMA that looks at what a single major Medicare Advantage insurer pays its providers.**
physician reimbursement in Medicare Advantage was more strongly tied to traditional Medicare rates than to negotiated commercial prices, although Medicare Advantage plans tended to pay physicians less than traditional Medicare. However, Medicare Advantage plans take advantage of the commercial market’s favorable pricing for services for which traditional Medicare overpays, including laboratory tests and durable medical equipment….
mean MA reimbursement ranged from 91.3% of TM for cataract removal in an ambulatory surgery center (CPT 66984; 95% CI, 90.7%-91.9%) to 102.3% of TM for complex evaluation and management of a patient in the emergency department (CPT 99285; 95% CI, 102.1%-102.6%)….
for laboratory services and durable medical equipment, where commercial prices are lower than TM rates, MA plans take advantage of these lower commercial prices, ranging from 67.4% for a walker (HCPCS code E0143; 95% CI, 66.3%-68.5%) to 75.8% for a complete blood cell count

This is a big, comprehensive study with very tight error bands. I find it persuasive with one caveat that I’ll get to in a minute. The big result is that the administrative prices set by Medicare Fee for Service matter a lot on procedure codes. Medicare probably currently overpays for labs and durable medical equipment.
I think this is good evidence that Medicare Advantage (MA) is able to get a better deal than Traditional Medicare (TM) because they have the ability to say no to providers. Medicare Advantage can create networks that are only enforced by cost sharing arrangements where they try to drive their members away from low value providers. From a policy perspective, this is a win as we want to force low value providers to stop being low value providers. That change is that they either go out of business or they get better or less expensive.
From a political angle, this finding along with other evidence that Medicare Advantage providers are getting fairly paid by the Federal government makes the long run case of a Medicare Advantage for all style universal coverage schema more plausible.
I do have one reservation about this study and it is the generalization of the findings.
And that is call the Senate.
Be firm, be polite and be clear about what you want your Senator to do about the BCRA.
Let them know that this is important to you, let them know it is important to your family and let them know it is critical to your community.
Open thread
Dean Baker and Brian Dew at CEPR write on ACA market structures. It is interesting but I don’t think they are thinking things through all the way. The ACA market structure, namely a price linked subsidy system where subsidy is a locally fixed sum tied to the second least expensive Silver plan in a region, creates oddities where simple analysis falls apart.
The lack of competition in the exchanges is a serious problem. While people can still buy insurance in the individual market off of the exchange, and still benefit from the ACA prohibition against discrimination based on pre-existing conditions, they are not eligible for ACA subsidies unless they buy insurance through the exchanges. These subsidies are necessary to make insurance affordable for millions of people.
So, the lack of a vibrant market in many counties is a serious issue for the ACA. However, there is an important part of the story that Trump and other Republicans forget to mention. The lack of competition in the exchanges is overwhelmingly a problem for people living in states controlled by Republican governors.
Competition is not an unequivical short term good for subsidized buyers. It becomes a micro level analysis. Competition in this type of marketplace produces odd results for subsidized buyers. We’ll work through some examples below the fold:
Kaiser Family Foundation has compiled the first quarter results of on-Exchange insurers and it looks good. The two graphs below are the Medical Loss Ratio (MLR) and the net claims versus net premiums for the quarter over time.

As you can see, MLR for the first quarter dramatically dropped. We’ll see what that means in dollars in a second:

Net premiums minus net claims is the wedge that pays for administrative costs and profits. That wedge is now almost $100. Well run, large insurers should be able to keep their admin costs down to $50 to $70 per member per month.
We need to be cautious about using first quarter data. This should be the best time of the year for an insurer for a couple of reasons. First, people are still going through their deductibles. The percentage paid by the insurer as a function of total allowed charges should be the lowest all year. This matters because deductibles and other cost sharing are both a way for insurers to shift costs back onto patients and more importantly, to reduce utilization. Some people will have known chronic conditions where they hit their out of pocket max in January or February every year and their incentives don’t change year over year. Other people have a surprise one time event such as when their cat attacks them after they are not fed for eight hour straight and destroys their shoulder. These people who unexpectedly maxed out have a strong incentive to get everything that they have been putting off for a while done in the rest of the year. They will have a spike of summer and fall claims.
Secondly, and more subtly, the population changes. Open enrollment will have just ended in the first quarter. This means the insurers are probably have the most people with low utilization on their books for the entire year. People will drop out of the pool. Those drop-outs will be due to natural movement (emigration, new jobs, marriages etc) and financial reasons (the premiums are too expensive). For the people who believe that their premiums are too much, they are far more likely to be very likely to be healthy than having significant care needs. New enrollees through the Special Enrollment Periods are either babies (expensive) or people who are willing to put up the time to go through verification and validation (so more likely to be sicker than average).
So what does this mean?
My first guess, having looked at both the Kaiser report and the financials of several insurers that I’m tracking, is that insurers slightly overcharged for 2017. They upped their rates by too much.
First quarter stability in the ACA marketsPost + Comments (13)
The Senate is back in town.
You know what that means.
Time to keep on calling the DC offices and the local offices and tell the interns answering the phones your strong, polite and coherently worded opinions on the AHCA/BCRA tax cut bills.
Andy Slavitt lays out the contours of the next two week:
Of all the many Senators who oppose the bill, McConnell is likely to press them 1:1 not to be the THIRD no if he gets that close. 11
— Andy Slavitt (@ASlavitt) July 9, 2017
The fundamental assumption in that tweet is that no Republican wants to by the decisive vote. The two allowable “No’s” have been taken by Heller and Collins. If there is a single vote left on the floor and the count is 49 Yes-50 No, the pressure will be immense to not be the person blamed for killing the bill. The bill will probably go to the floor if McConnell can count on 47 or 48 solid Aye votes. He figures he can arm twist and allow a political pressure cooker to squeeze the last few people whose personal political preference is “Vote No, hope yes but is there if needed.”
So that means the hard No’s need to be locked down. So people from West Virginia, call Senator Moore Capito; people from Kansas call Sen. Moran. Keep on calling.