My only hope for the new year is that 2017 is not telling 2016 “hold my beer and watch this…..”
Open thread
![]()
Come for the politics, stay for the snark.
I am a student in the doctoral program at the Duke University Department of Population Health Sciences. I am working towards my my doctorate in Health Services Research with a policy focus. I am fundamentally fascinated by insurance markets, consumer choice and the navigation of complex choice environments. I'm currently RA-ing at the Duke Margolis Center for Health Policy.
I used to be Richard Mayhew, a mid-level bureaucrat at UPMC Health Plan. I started writing here and have not found a reason to stop.
Conflicts of interest: Previously employed at UPMC Health Plan until 12/31/16. I also worked full time as a research associate at the Duke University Margolis Center for Health Policy. I have received direct funding from the National Institute for Healthcare Management, and I have been on projects funded by the Rockefeller Foundation, Kate B. Reynolds Charitable Trust, Gordan and Betty Moore Foundation, Duke University Health System, CMMI, and various value based payment consortiums. I serve as a consultant on a grant from the Commonwealth Fund and have acted as a consultant to several ACA insurers.
Research Production is here: https://scholar.google.com/citations?user=zof9b4IAAAAJ&hl=en
David Anderson has been a Balloon Juice writer since 2013.
My only hope for the new year is that 2017 is not telling 2016 “hold my beer and watch this…..”
Open thread
I am not an economist. I am not trained as one. I do not play one on the blog. But I have a health policy question with potential macro-economic implications?
What effect does a low actuarial value/catastrophic coverage paired with Health Savings Accounts (HSA) regime have on national savings?
Insurance (of any sort) has two major economic value propositions. First, it pools risk so that unpayable costs become payable. This encourages productive risk taking in the face of tail risk. Secondly, because of the pooling function, it reduces the variance faced by any individual in the pool. Lower variance means more predictability which means less uncertainty. Properly priced insurance will lead to lower net social savings as the risk is distributed and people are not in a position to be run over by a five sigma event.
A good real world illustration is the Chinese savings rate. China (as of 2015) has a massive savings rate. The country as a whole saves roughly 50% of GDP. Some of this is due to a government decision to tamp down on consumption in order to fuel investment. A good portion however is due to the immature insurance market. People can not easily buy good health insurance, so they save in case a family member gets cancer. People can not buy long term annuiuties to protect their retirement against the risk of living long and well, so they save. People are attempting to self-insurer. Each person or each family becomes their own risk pool and their own absorber of tail risk. The vast majority of people never get hit in the face by their tail risk, so they effectively oversave while the people who are hit by tail risk are still screwed as they can’t save enough given average lifetime earnings.
The Chinese government is moving towards national social insurance partially in order to reduce the savings rate and increase domestic consumption. People who are hit with extreme tail risk will be better protected while the average person will pay a little bit less to get the same protection. Net society-wide savings, all else being equal, will decline.
Now let’s move over to the HSA world that we may be entering. The theory of change is that people will be price sensitive to their basic medical care as they’ll pay for it directly with pre-tax personal dollars which could otherwise be rolled over into future years. This will lead to both lower utilization and more cost effective utilization which will bend the cost curve while also improving the quality of care. I’m skeptical of those outcome claims but that is irrelevant. Out of pocket maximums for some of the plans floating around start at $10,000 or more as the minimal acceptable level of coverage (55% AV) and go higher depending on the plan we look at. After that, insurance would kick in to cover hit by a meteor coverage. What does this do to net savings?
Macro-economic effects of an HSA regime?Post + Comments (70)
Let’s talk risk adjustment and the problem with averages. The picture below is two hypothetical diseases with twenty patients where the average cost to treat is $1,000 per year for each condition. However the spread in the cost varies. Condition A is tightly clustered while Condition B has a very large spread between the low cost members and the very high cost members. What does this mean for risk adjustment and cherry picking?
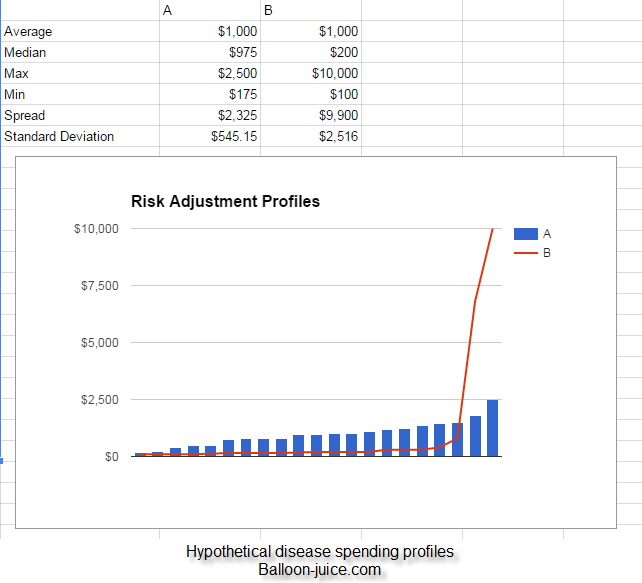
These two diseases have the same average incremental cost to treat ($1,000) but applying similar risk adjustment to these diseases will produce very different insurer behaviors.
Let’s review risk adjustment before we figure out why insurers will respond to the same method depending on the disease profile. Risk adjustment counteracts the simplest way to make money as an insurer. Insurers can make a lot of money by charging high rates to low risk people while running far away from high risk people. That can be okay in insurance systems where we as a society do not care that everyone is covered. Travel insurance or auto insurance will be good examples of this. However for health insurance in a world of guarantee issue and community rating with multiple payers which is most government sponsored health insurance market groups (Medicare Advantage, CHIP, Medicaid managed care, Exchange) this is a major issue.
The optimal strategy for any individual insurer in a world without risk adjustment is to collect the average premium without taking on average medical risk. This logic produced the Gresham law race to the bottom for AIDS drug benefits where ugly plans drove out attractive plans from the market.
Risk adjustment is the counter to this individually rational but market destroying behavior. In the simplest form it is an attempt to give more money to the insurers that have higher medical risk. Ideally, it should move money around in a way that insurers are fundamentally indifferent to the medical risk that they bear so that insurers then compete on their provider costs, networks, benefit design, member services, and disease management capabilities. Risk adjustment can be bump payments with external funding (Medicare Advantage does this) or inter-insurer revenue neutral transfers where insurers with healthily coded risk pools send money to insurers with sicker than average coded risk pools (Exchange and at least some Medicaid managed care states).
The size of the payments can be either a proportion of average premium times a multiplier or a lump sum transfer. Medicare Advantage gives a lump sum payment to the insurer for each diagnostic category. Exchange will take a multiplier of the average premium in a state and use it to calculate the individual insurer’s relative risk.
So now that we covered the basics, how would insurers react to these two disease profiles? Disease A is tightly clustered. The spread is a little more than twice the mean and the median is almost the mean. The most expensive patients are not extreme outliers compared to their peers. An insurer would love to get all of the low cost members with Disease A and pocket the risk adjustment transfers. The insurer would profit as the transfer payments are more than the cost of actual treatment while their competitors would be holding the bag on the few above transfer payment cost to treat individuals. But the amount of money that could be gained by successfully skimming the risk pool is not substantial.
Disease B is a very different profile. It has the same average cost as Disease A but the distribution is very different. Eighteen of the twenty individuals have costs that are less than the average costs. Two individuals have costs substantially above the average ($5,000 and $10,000) so 10% of the pool is driving 75% of the costs. This is not atypical as health care is a Pareto industry.
A flat bump payment produces very bad incentives.
Insurers would compete vigorously to get the bottom 90% enrolled as these members are profit centers after risk adjustment. The problem is that every insurer is going to run like hell from the two high cost members. They are guaranteed money losers. This means networks will get cut, drugs will be placed on high cost sharing portions of the formulary and every other barrier to enrollment will be set up. If a carrier in the first year gets a large number of the very high cost individuals within a disease category they will change their offerings to make it ugly in the second year.
This incentive can be beaten if there is two part risk adustment. The first part would be a bump payment or a base score for relative risk calculation purposes that effectively covers the standard of care for the eighteen low cost individuals. The second part is a catastrophic reinsurance or bonus score for relative risk calculation that only applies to individuals with certain procedure codes and documentation. At that point, the incentive to run like hell from the sick and cherry pick the risk adjustment gold mine is minimized at the cost of higher administrative complexity.
Later on this week, we’ll talk about concurrent and adjusted period risk adjustment and the challenges both try to solve.
From McClatchy we sit a clear trade-off between making sure kids are healthy and able to contribute to a bright future or high income tax cuts:
4.4 million children could lose health coverage in 2019 if the Affordable Care Act is partially repealed through the budget reconciliation process, according new report by the Urban Institute, a progressive, non-partisan think tank.
Likewise, the uninsured rate for … children would more than double in 2019 from … from 4.1 percent to 9.6 percent for children under age 18, the report found…
Of the 4.4 million children who would lose coverage in 2019, 88 percent would have working parents
The previous ACA repeal bill also allowed states to lower child eligibility levels for Medicaid and the Children’s Health Insurance Program (CHIP) beginning in 2017. If all states did so, another 8.9 million children would be without coverage in 2019
So we’re looking at between 4 and 13 million children being sacrificed to the altars of Moloch.
Good to know.
Uninsured rate among <18 with repeal.
1998: >16%
2016: <5%
2019: 10%I see a problem.https://t.co/1yDWR1qNEb
— Andy Slavitt (@ASlavitt) December 22, 2016
And we call ourselves civilized.
I want to highlight something that bothers me about the entire idea of getting massive cost savings from emergency room diversions (via TPM):
The example Rep. Bill Huizenga (R-MI) gave in an interview with MLive.com was from his own experience when he waited until the morning after to take his youngest son to the doctor with an injured arm, because he did not want to waste money on an expensive emergency room visit. The arm, it turned out, was broken.
“We weren’t sure what was going on. It was in the evening, so I splinted it up and we wrapped it up, and the decision was, okay, do we go to the ER? We thought it was a sprain, but weren’t sure,” Huizenga said, adding that he and his wife “took every precaution and decided to go in the next morning.”
“When it [comes to] those type of things, do you keep your child home from school and take him the next morning to the doctor because of a cold or a flu, versus take him into the emergency room? If you don’t have a cost difference, you’ll make different decisions,” he said.
I hate this example for a lot of reasons including the fact that a broken bone is a legitimately good reason to go to the emergency room. It is a source of significant pain, significant impairment and over time a simple break left untreated can lead to a complex set of breaks that requires very expensive surgery. But that is besides the greater set of points why this is a bad story to tell.
Let’s go back to the most important graph in healthcare:
Why consumers won’t drive the #healthcare market. Most costs from high $ people who are beyond cost sharing. pic.twitter.com/buoAM00CPT
— (((Martin Gaynor))) (@MartinSGaynor) December 10, 2015
ER utilization can be broken into three components. True emergencies that lead to admissions. Here ER utilization is expensive but very valuable. Then there are acute emergencies that occur either off hours or can not be handled at the PCP or Urgent Care office due to the lack of equipment where the ER may not admit but they are an appropriate resource. Asthma attacks and broken bones are common pediatric examples of this case while unspecified chest pains and shortness of breath are good examples of older people. And then there are the cases where the ER is overkill. The problem is that ER overkill is a real problem but it is not a big driver of total medical spending. It might be a $5-$10 per member per month in the most aggressive modeling.
Marginal ER utilization for flip a coin decisions where having a large deductible could drive people to wait a day or two before getting a broken bone treated is not that big of a deal. Those are the cases on the left hand side of the graph. People who don’t use the ER a lot, who don’t use a lot of services a lot don’t cost the system a lot of money. Shifting a single in-network medium severity ER visit to a single in-network medium severity Urgent Care visit might lower the contract expenditure by $200 or $300. If the kid’s arm is broken and it needs surgery, that is 5% of the total episode of care cost. If there is nothing beyond an “oowie”, the shift might save 75% of the episode cost of care. The shopping paradigm is that it will change behaviors among people who are not driving most of the healthcare spending. It will save money but it is limited in what it saves as the people use a lot of medical resources will blow through any out of limit cap very quickly.
And this story only makes sense if there is a significant substitution effect between ER and Urgent Cares.
Researchers race to copy Obamacare data for fear it will vanish https://t.co/vg1KvReTzr via @ddiamond pic.twitter.com/qiF379l3Uh
— POLITICO (@politico) December 21, 2016
I’ll be downloading everything that I can from Healthcare.gov by January 15th.
I hope that I’m wasting my time but the cost benefit analysis is clear that downloading and archiving is a plausible choice. In the best case scenario, I waste my time. It is only two weeks on the clock while I build a deeper understanding of the entire data universe. I’ve wasted two weeks on projects that had no pay-off before and I know that I will be on projects that go nowhere at some point again in my life. I will have learned something and brought into local control useful data that I can bounce off of national data. Best case scenario, I incur minor costs that are slightly higher than minor benefits.
It is the worst case scenario where data just gets either locked down or yanked from the public and is only accessible via FOIA requests in non-user friendly formats that the pay-off is strong. Again it is two weeks of my life but it is access to years of research material that can fuel impactful analysis. It would be the creation of health policy wonk trading sub-culture that rivals show tapes of Deadheads — I’ll trade you a 2014 Rate PUF for a 2009 CBO public option report man….
And if you assume that this worst case scenario has more than a 1% chance of happening, that is a very good use of a few weeks and a few gigabytes worth of space.
I have to assume environmental and consumer protection focused folks are doing the same thing, just in case.
"Trump will destroy Medicare and Social Security" might do, as it appears to be true. https://t.co/Ign6jX3esH
— xpostfactoid (@xpostfactoid) December 20, 2016
I love my parents. One of the smartest and best things that I did for my relationship with them was moving six hundred miles away for college as I was a complete snot as a teenager. The distance allowed me to be less of an idiot while growing up without having them as a locally convenient authority figure to mindlessly but loudly rebel against.
One of my great pleasures as a parent is seeing my parents be grandparents. My mom tried to go bowling with the grand kids a few weeks ago. My dad spent most of a morning helping my son build a model so that it fly around the kitchen and living room while they tried to rescue stuffed animals and plastic figures. I laugh when I see my kids do something that harkens back to the grandparents’ curse — “May your children be just like you”. I look forward to calling home and telling my mom about what her granddaughter just did as I wait to hear her laugh at and with me.
I want them to visit. I want them to spend a week or two. I want them to be a part of my life and my kids’ lives. I want them to introduce the idea that ice cream can be dinner when it is Grandma’s Rules.
I also don’t want them to live with us as they age.
This I think is powerful messaging as to why the defined benefit nature of Social Security and Medicare need to be kept. I’m not a marketing person, but I think this is a valuable element.
Love you, don’t want to live with you Mom and DadPost + Comments (268)