

The Biden administration has made the biavelent booster free, widely available, and have been talking about it constantly.
You would think that after 3 years, you nerds would've learned a thing or two about the public. People being over COVID is not the fault of the gobmint. https://t.co/kEKz0YG9L6
— What Biden Has Done (@What46HasDone) December 31, 2022
=====

(link)

(link)
(link)
How deadly will China's #Covid surge get? Experts tackle that question as well as these: How fast is the virus spreading there? How long will the surge last and will China spawn a new variant? https://t.co/nB60leukFW
— delthia ricks 🔬 (@DelthiaRicks) January 1, 2023
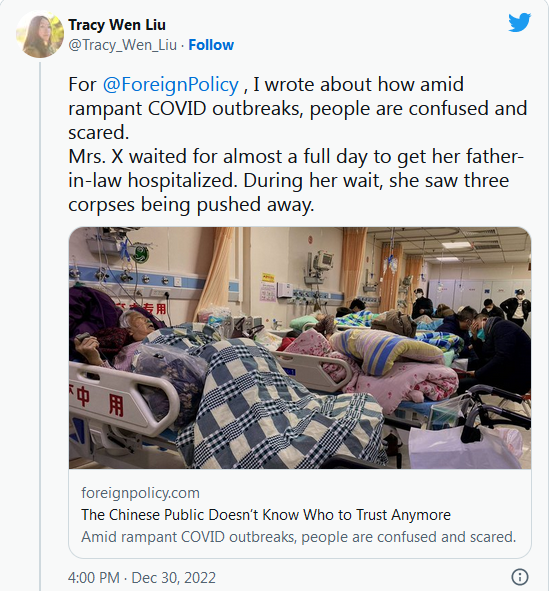
This is a good human-interest article, but the part that raised the hairs on the back of my neck…
… A doctor from Wuhan who worked on the front line during the initial outbreak of the pandemic in 2020 told Foreign Policy, asking for anonymity, “We are not against opening up, but we are against opening up in this manner.” She said that the hospital was not prepared when all COVID prevention and control policies were lifted. According to her, COVID screening was not required anymore. This ensured that patients with COVID could be accepted and treated, but it also made it impossible to separate patients with or without COVID infections, which could lead to cross-infection in the hospital ward. In scenes reminiscent of early 2020 in Wuhan, patients flooded into the hospital, but it was not equipped with sufficient medicine and protective gear, which led to a severe shortage of medical resources.
According to the doctor, many medical workers are infected as well, worsening the situation in the hospital, and they, too, are unsure of the proper treatment. After catching COVID, she suffered from a high fever and shortness of breath for weeks, but she was called back to work after a week, before she had fully recovered.
She told Foreign Policy that many patients’ CT scans showed severe lung inflammation, while it is commonly believed that the omicron variant appears to cause less damage to the lungs. Many patients she saw also suffered from serious breathing issues, which was not common among people who contracted the omicron variant. She has heard various opinions. Some medical experts suspect that Chinese patients are suffering from more severe symptoms because the vaccines they received provide less protection, and some experts suspect that there is a new variant, but she isn’t sure what to believe.
In the past few days, the term “white lungs,” which refers to CT scans showing severe lung inflammation, has trended on Chinese websites and people are speculating that patients with white lungs were infected not with the omicron variant but with a previous variant or even the original strain that was spreading in Wuhan in early 2020. On Dec. 27, Jiao Yahui, director of the Department of National Health Commission’s Medical Administration Bureau, said in a media conference that “white lungs” have nothing to do with the original COVID strain or vaccination. However, people don’t seem to be convinced by this statement. Some of them have lost trust in government assurances and medical experts.
It’s a problem across almost all areas of Chinese life, not just health care. With government data now nonexistent or actively falsified, it’s hard for people to evaluate risk. Even if they are aware of the catastrophe unfolding in hospitals, just how severe new variants might be—or how effective the Chinese vaccines are—is impossible to know. The rich are now rushing to Macau for mRNA shots and buying up Paxlovid online; the rest of the public has been left to struggle on its own.

(link)
(link)

(link)
Canada:
The AREA UNDER THE CURVE from the end of November 2021 to the present dwarfs the period from April 2020 to November 2021. So, in what way precisely is the pandemic "over"?
— Dr David Berger, aBsuRdiSTe cROnickLeR (@YouAreLobbyLud) December 31, 2022
======
“If you make a big bet, and you’re successful with a program [Operation Warp Speed], you should keep making big bets"https://t.co/zHVRYmP4vW @SmithsonianMag by @SimarSBajaj
— Eric Topol (@EricTopol) December 31, 2022
I've added a map page to my dataviz on COVID-19 genomic sequencing data.
Here I've used it to visualise the spread of the new XBB.1.5 "Kraken" lineage around the world.https://t.co/FuHOL8g6Xg pic.twitter.com/gXZ2l8EuEn— Mike Honey (@Mike_Honey_) January 2, 2023

(link)
(link)
#Covid has been linked to a crippling heart condition called 'PoTS.' Most experience it as a #LongCovid symptom. Acronym means Postural tachycardia syndrome, an abnormal leap in heart rate when sitting up or standing. Patients can become dizzy or faint. https://t.co/WVuju8G5lV
— delthia ricks 🔬 (@DelthiaRicks) January 1, 2023

(link)
#Covid pill studied in clinical trials in China may be an improvement over Paxlovid. Drug is a remdesivir derivative developed in China. Remdesivir is a US product. Experimental drug—VV116—worked well in high risk patients. Remdesivir's chemical structure⬇️https://t.co/0RfoPJpkpZ pic.twitter.com/4STHJ1I9Qq
— delthia ricks 🔬 (@DelthiaRicks) December 30, 2022
======
We should not be going back to the drawing board or trafficking in hysteria every time a new subvariant emerges. Instead, we need to achieve high, equitable coverage of the tools we have and activate short-term mitigation tools to blunt the impacts of surges.
— Anne Sosin (@asosin) January 2, 2023
(link)
Yale (Connecticut):
While outcomes are dramatically better & #COVID19 does not affect the hospital’s function, need to #StaySafe. You know the drill.
Get COVID bivalent & Flu vaccines
Reduce exposures, #MaskUp in indoor gatherings, use ventilation
Get tested & treated if indicated #COVIDIsNotOver— Naftali Kaminski (@KaminskiMed) January 2, 2023
I know, I know – we were supposed to "focus protect" the at-risk. I made that exact argument in spring 2020. But in a city like NY, you have millions of at-risk citizens, most of them living on their yen or in multi-generational households. How do you "focus protect" them?
— James Surowiecki (@JamesSurowiecki) December 31, 2022
For those who keep saying they don't understand why we are so focused on masks: Mask mandates are the policy that would instantly make a huge difference to the lives of higher risk people. It would mean they could go on public transport, access medical care, & other basic needs.
— Dr. Lucky Tran (@luckytran) January 2, 2023
Masks aren’t perfect, no one single measure is, which is why we need to keep advocating for multiple measures including ventilation, next gen vaccines, and better treatments.
But we are in a surge now that is keeping our most vulnerable locked out of society. We can’t keep people at home indefinitely, unable to access essential needs. Mask mandates will instantly open up society to millions more people, while we work on longer term solutions.
If we give up on mask mandates and universal masking now, that would mean millions of higher risk wouldn’t be able to fully participate in public life for years. That’s unacceptable.
We’ve been gaslighted by leaders into accepting policies that don’t solve the pandemic because they hurt the people who are most vulnerable and lock them out of society. We can do better.
To end the pandemic we need measures that actually reduce COVID spread, like ventilation & better vaccines. These measures will take time to come into effect (they can happen faster if we speak up). In the meantime, mask mandates will open up society to more people & reduce harm.
There is no “apolitical” way out of this pandemic. It’s a political choice to accept policies that continue mass death and exclude people from society. We can only turn things around if we fight for more equitable policies. That means speaking up for all protections, inc masks.
 On The Road – StringOnAStick – Backcountry skiing, Monashee Mts, B.C.
On The Road – StringOnAStick – Backcountry skiing, Monashee Mts, B.C.{kind=link}
Reader Interactions
41Comments
Comments are closed.
YY_Sima Qian
Lack of consistency in the availability of meaningful data continues to pose challenges for developing a clear picture of the exit tsunami in China. The daily dumps that the China CDC publishes is still meaningless in relation to reality, although even that data has shown rapidly increasing severe/critical cases over the past week (the absolutely number, at 3,305, is probably orders of magnitude lower than reality). Local Chinese authorities have been filling the gap w/ thrown releases of survey and modeling results. Sichuan Province announced on 12/26 that > 63% of residents surveyed have either tested positive on PCT or RAT, & another 30% had COVID-19 symptoms but did not test. Hainan Province announced on 12/30 that ~ 50% of residents have been infected. Quzhou in Zhejiang Province announced on 12/28 that ~ 30 – 35% of the residents have been infected, while Zhoushan in the same province announced on 12/29 that ~ 30 – 40% of residents have been infected. Baidu’s model continues to believe that all but a handful of outlying cities/prefectures in China are already past peak in infection.
There is no good way to assess the picture for severe/critical cases, other than anecdotes from personal contacts & social media, but at least the cities at the front of the exit tsunami should be peaking or have peaked. We tried to move my wife’s grandparents to one of the top hospitals in Wuhan, leveraging every contact we have, but the answer was always no, there are no beds available there. At the same time, two of our elderly distant relatives became infected over the weekend & developed a cough. They were admitted into a hospital as a precaution. This would not have been possible a week & half ago, since their symptoms do not require hospitalization & there were no beds to be had in any hospital back then. That suggests to me that hospital beds are now becoming available in Wuhan (except for the handful of the best ones in the city), as recoveries + deaths now outpace new severe/critical cases. There is no longer a significant wait time for ambulances here. Hospitalizations may be approaching peak for the next echelon of cities (such as Shanghai & Nanjing) behind the front of the exit tsunami. My relatives in Nanjing who are doctors & nurses expect the next few days to be the peak for severe/critical cases.
Through the exit tsunami, hospitals in China could no longer attempt to separate COVID-19 & non-COVID patients in nosocomial settings. Every ward has a mix, & most patients come in positive w/ SARS-CoV-2, whether COVID-19 is the cause of hospitalization or not. Most of the medical staff have been infected, as well, whether in the hospital or in the community. Those w/ mild to moderate symptoms are asked to continue to work, or the hospitals would not have any people to staff them. My doctor/nurse relatives tell me that every medical staff in every department in every hospital have been trained to treat COVID-19 (or at least to alleviate the symptoms), since every patient either comes in positive or is likely to become positive shortly into the hospital stay.
In the meantime, as the vast majority of the urban populations of major Chinese cities have recovered in the past couple of weeks. socio-economic activity is recovering rapidly. Every city saw tens to hundreds of thousands gathered at major landmarks to watch fireworks & ring in the New Year. ~ 300K people gathered on the banks of the Yangtze River in Wuhan. Even though many cities have banned private fireworks (for fear of fire hazards & pollution), people have universally ignored the ban, much to the frustration & chagrin of the police & fire department. Many people around us have gone on revenge travel during the New Year long weekend, especially those from the cold northern China going to the warmer southern & southeastern coast. Hotels at popular tourist destinations in souther China are fully booked for the Chinese New Year “golden week” holiday. It appears after over 6 mo. of uncertainties & inconveniences associated w/ trying to contain Omicron, plus a mo. of anxiety associated w/ mass infection, many are looking for release. At least masking rate is still nearly 100% even outdoors.
All signs point to an incredibly intense, but also very short, exit tsunami in China. We should expect similar trend for severe/critical cases & deaths.
Having kept mum throughout the massive wave of infections & rapidly rising hospitalization/death, the central government is start to comment on the exit tsunami, however obliquely. Officials at the China National Health Commission just did an interview w/ China Central Television that discussed the dire situations seen through the exit tsunami. In it, the China NHC acknowledged that the intensity of the tsunami greatly exceeded the capacity for fever clinics, hospital beds & ICUs. They described how the 1st part of the health care system to be pressured was the fever clinics, followed by the ERs, then the ICUs. They reemphasized that the percentage of severe outcomes is very low w/ Omicron, but the stress comes from the very large base of infected persons during the exit tsunami. They also acknowledged that they do not have great visibility as to how large that base truly is, due to the end of mass screening, & that they can only rely upon surveillance testing & modeling. In his customary New Year’s address, Xi Jinping also acknowledged the difficulties that Chinese people endured in 2022, & the fact that “1.4B people will naturally have different opinions/perspectives & different desires”. Previous New Year addresses have been unabashedly triumphant in tone. This year’s speech is still focused on China’s & the CCP Regime’s accomplishments, & Xi emphasized the need to forge consensus despite the variety in opinions & desires. Nonetheless, it is notable that Xi had to acknowledge the diversity of opinions & desires int he 1st place. However, there has been no let up in censorship, or harassment/arrest of those who took prominent positions during the protests at the end of Nov.
As of 1/2, 3,478.946M vaccine doses have been injected in Mainland China, an increase of 458K doses in the past 24 hrs. As of 12/13, 1,307.222M individuals have taken at least 1 shot (or 92.73% of the total population), 1,274.018M are fully vaccinated (90.37% of the total), & 815.718M boosted (57.86% of the total). Of the > 60 y.o. cohort, 240.217M individuals have taken at least 1 shot (or 91% of the cohort), 228.644M are fully vaccinated (86.6% of the cohort), 184.179M boosted (69.76% of the cohort). Of the > 80 y.o. cohort, 27.73M individuals have taken at least 1 shot (or 77.5% of the cohort), 23.757M are fully vaccinated (66.4% of the cohort), 15.153M boosted (42.35% of the cohort).
On 1/2, Hong Kong reported 16,186 new positive cases, 324 imported & 15,862 domestic, & 75 new deaths. There have been 11,943 total COVID-19 deaths to date.
On 1/1, Macao reported 78 new cases & 5 new deaths. There have been 52 total COVID-19 deaths to date. The Macanese authorities believe ~ 50% of residents have been infected to date.
On 1/2, Taiwan added 25,009 new positive cases, 360 imported & 24,649 domestic. There were 22 new deaths. There have been 15,321 total COVID-19 deaths to date.
YY_Sima Qian
On a more personal note, my wife’s grandparents remain in the hospital, but seem to be improving. The doctors started a course of Azvudine for the grandfather. It is a reverse transcriptase inhibitor, approved for EMU in China in Jul. 2022 for COVID-19, & approved for conditional use to treat HIV infection in 2021. Unfortunately, no clinical data have been released for either use. The grandmother is actually testing negative now, mostly symptom free, & is eligible to be discharged. My uncles & aunts in Beijing & Nanjing have all recovered from their infections, but some are suffering from common short term sequelae (persistent coughs, lethargy, cold seats, etc.).
Unlike so many around us, we plan to take it easy until after Chinese New Year. XBB.1.5 is already in China, & w/ its immuno-escape properties & good fit for hACE2 receptors, the recent BA.5.2/BF.7 infection may not offer that much protection.
Amir Khalid
Malaysia’s Ministry of Health reported 360 new Covid-19 cases yesterday, for a cumulative reported total of 5,027,457 cases. 359 of these new cases were local infections; one new case was imported. It also reported one death, for an adjusted cumulative total of 36,858 deaths – 0.73% of the cumulative reported total, 0.73% of resolved cases.
20,253 Covid-19 tests were conducted on 31st December, with a positivity rate of 3.8%.
There were 11,807 active cases yesterday, 64 fewer than the day before. 580 were in hospital. 30 confirmed cases were in ICU; of these patients, 16 confirmed cases were on ventilators. Meanwhile, 423 more patients recovered, for a cumulative total of 4,978,792 patients recovered – 99.0% of the cumulative reported total.
The National Covid-19 Immunisation Programme (PICK) administered 2,919 doses of vaccine on 2nd January: 53 first doses, 37 second doses, 314 first booster doses, and 2,515 second booster doses. The cumulative total is 72,570,216 doses administered: 28,120,894 first doses, 27,532,308 second doses, 16,280,153 first booster doses, and 636,861 second booster doses. 86.1% of the population have received their first dose, 84.3% their second dose, 49.9% their first booster dose, and 2.0% their second booster dose.
New Deal democrat
Biobot has not updated since late last week, but shows the biggest nationwide outbreak since Omicron one year ago, and slightly bigger than all other outbreaks. Regionally the Northeaat continues to be the hardest hit, followed by the South, then Midwest, and finally West, where cases are relatively low and increasing only slightly.
*Confirmed* cases are probably still affected by non-reporting over the holidays. They are at 52,100, relatively low for the last 9 months, and have declined in all 4 Census regions in the past week. They remain the highest in PR, NY, NJ, and southern New England. They are the lowest in the Northern Mountain States, the Pacific Northwest, the Dakotas and ME.
Hospitalizations continue to increase sharply, up 20,000 in the last 6 weeks to 45,300, only 2,000 below this past summer’s BA.2.12.1 peak. Deaths, at 337, are probably also affected by holiday non-reporting.
The latest booster shot is reported to remain effective against XBB.1.5, which increased sharply to 45% of all cases as reported last Friday by the CDC.
OzarkHillbilly
That top comic… Just gotta say nobody ever accused me of being a “wise” man, just not a complete idiot.
YY_Sima Qian
“White lung” is indeed a topic of conversation in China. The lack of the protection offered by recent boosting may be a contributing factor. However, I think people keep forget how many people there are in China, & have failed to appreciate just how quickly COVID-19 has spread in the exit tsunami. Even if Omicron BF.7 (the strain prevalent in northern China) does not produce higher percentage of severe lung infections in China than elsewhere, the fact that so many people have been infected so quickly, a tiny percentage of a huge number ends up being quite a large number.
NeenerNeener
Monroe County, NY:
130 new cases on 12/30/22.
110 new cases on 12/31/22.
107 new cases on 01/01/22.
82 new cases on 01/02/22.
Deaths at 2127, up 7 from last week.
As for hospital beds, only 3% are actually available, including 11 ICU beds among 4 hospitals. The largest hospital has no available beds, and the second largest hospital only has 17 beds available.
I had to leave my house and go to a medical lab twice for scans last week, and now I’m dead tired all the time. My COVID tests keep coming back negative so far though.
catclub
So I have moved from one state to another. Who has my vaccination record?
Princess
I like the name “exit tsunami.” Makes it sound like an unstoppable force of nature against which no human interventions or mitigations are possible, whereas of course they are/were. My guess is that’s the point of the name.
Anyway I’m salty this morning because a militantly anti vaxx relative has caught Covid as was entirely predictable, threatening his unvaxxed family, including his frail elder relative who lives with them. Trying to push paxlovid but my guess is he’ll refuse anything but ivermectin..
catclub
@catclub: answer is MyIR records for old state.
YY_Sima Qian
However, I am disappointed (but not surprised) at the Foreign Policy article. Lack of meaningful data is understandably causing anxiety in Chinese population & even Chinese medical professionals. However, beyond simply reporting on & echoing that anxiety, Foreign Policy should be able to access more expertise than the average person in China can. Like reporting that the countries that have tested & sequenced travelers from China have confirmed that the strains currently prevalent in China are indeed BF.7 & BA.5.2, & not ancestral variants long outcompeted by Omicron, nor some newly brewed Omicron strain.
This failure to educate or inform characterize far too much of MSM on far too many topics.
rikyrah
Continue to be shocked at what appears to be the lack of preparation for COVID reopening in China 🤔
YY_Sima Qian
@Princess: You know, if you want to insinuate bad faith on my part, just come out and say it, instead of passive aggressive BS.
Matt McIrvin
It seems like there’s a lot of worry about the Chinese exit wave hitting here, but our big problem right now is XBB.1.5, whereas the Chinese wave is mostly variants that hit us months ago, have already been circulating for some time in the US and are subsiding. We’ve probably got much more resistance to them. They should be worried about US.
I’m back to watching the wastewater updates in suspense. A bunch of people I know got COVID over the past couple of weeks. Is this going to be as big as the winter 2021-22 Omicron wave or not? There are indicators that you can read either way. It could be smaller or it could just be happening a couple days later; that’s the trouble with exponential growth–you can’t tell the difference just by eyeballing charts until it actually turns over.
Soprano2
@catclub: If you’re talking about Covid, you have it on your vaccinate cards. I’ve told my doctor when I get boosters, but I don’t know if they’re recording it in my medical records or not
Our last sewer testing update was 12/19, which showed a small uptick at the larger plant, but still well below the last peak.
YY_Sima Qian
@Matt McIrvin: I assume vaccine booster shot & Omicron infection still confer T-cell & B-cell immunity, so XBB.1.5’s immune-escape properties may induce another huge wave of infection, but probably not an equivalent wave of hospitalizations & deaths as the Omicron wave in winter 2021-22. Of course, every COVID-19 wave seems to cull some (steadily decreasing) percentage of the vulnerable population, including those vulnerable by choice (through foregoing updated boosters in a timely fashion).
Soprano2
I understand Dr. Tran’s advocacy for mask mandates, but all you have to do is read the comments underneath those tweets to understand that mask mandates are NEVER coming back in the U.S., at least in many parts of it.
Matt McIrvin
@YY_Sima Qian: What I’m seeing right now looks very different depending on what you look at: local hospitals seem to be less crammed than they were, ICU hospitalizations are much lower, but hospital admissions have gone up alarmingly in the past couple of weeks, in some cases as high as in the equivalent stage of the Omicron wave.
Maybe that’s in part because they don’t have as many beds filled already and are more willing to admit people instead of telling them to ride it out at home. Maybe the wider use of Paxlovid and better treatments in general are keeping people out of the ICU and keeping the hospital stays shorter. Hard to say. I’m not seeing a wave of “crammed hospital” stories yet… except that I’ve heard about pediatric wards struggling with RSV, flu and COVID hitting at once.
Deaths are increasing but that’s such a noisy and lagging indicator that it’s hard to tell much.
PIGL
@Soprano2: I’m not sure that such a strong conclusion is supported by the hysterical ravings of internet anti-vaxxers.
New Deal democrat
@Matt McIrvin: 91-Divoc has a useful tool for tracking the 2nd derivative, which will give you evidence of exponential spread: the one week change in the one week average, including a per capita option.
Since NY, NJ, and parts of New England have 70% penetration by XBB.1.5, it ought to be visible. Although we are definitely hampered by lack of daily updating by States over the holidays, at this point unless I missed it it doesn’t appear to show anything even remotely close to last year’s Omicron spike.
Hpoe that is helpful.
Ella in New Mexico
@catclub: the state you got them in, we don’t have a national data base unfortunately.
This has always been a frutration for things like proof of vaccination for school attendance, but seems like this should have been addressed in the big Omnibus bill with a quite line item.
YY_Sima Qian
@Matt McIrvin: It could still be consistent. I think one of the key attributes of Omicron variants is very rapid replication w/in the body, which can get everywhere inside of the body. Since the XBB.1.5 has immune-escape characteristics relative to the BA.5.X strains, the antibodies induced by BA.1/2/5 targeted bivalent booster or recent BA.5.X infection cannot effectively neutralize XBB.1.5 virus upon introduction into the body. So the virus replicates very quickly & in some percentage of cases it can cause symptoms serious enough as to require hospitalization. However, the T- & B-cell immunity conferred by the vaccine shots and/or prior infections means the body still response quickly enough & defeats the virus before symptoms progress to the worst outcomes (except for a decreasing small percentage of the most vulnerable, whose immune systems are weak & forgetful). That is my WAG, anyway.
Matt McIrvin
@New Deal democrat: The wastewater shows an exponential rise that’s running, just going by eyeball, about 40-50% of the first Omicron spike at the same time a year ago. But, as I said, that could just be down to a short delay–it’s impossible to say yet.
The case counts are not consistent with that, but I think the case counts are not credible and can just be ignored. Hospital admissions are consistent with that, broadly speaking.
The Moar You Know
Per Al-Jazeera: “The United States, Canada, Japan and France are among countries insisting all travellers from China provide negative COVID-19 tests before arrival, as concerns grow over a surge in cases.”
Apparently China feels these restrictions are unacceptable, but all their restrictions on incoming travel were not. They really are trying to be the America of the 21st century, aren’t they?
Fair Economist
Influenza Summary for week ending Dec. 24, 2022;
Summary: Influenza down but still at epidemic rates. Respiratory mortality rising and above pre-COVID peaks.
Flu lab positivity down from 24.4% to 19.8%. Visits for influenza-like illnesses (ILI) down from 6.3% to 6.1%. Flu hospitalizations from 20,783 to 18,848. Respiratory mortality up from 12.0% to 12.1%.
Flu types are overwhelmingly Flu A (99.5%) with H3N2 being the large majoriy of those (77.8%). After missing last year, the flu vaccine seems to have hit the mark this year with the predominant H3N2 strain almost exclusively the strain used for the vaccine. Yay! Also, all flu viruses tested this year have been susceptible to all flu treatment drugs, so yay there too.
Generally speaking, areas hit early with high ILI rates like GA and TN are seeing declining rates, likely reflecting dropping flu rates and predicting further declines in flu for the rest of the country. NYC is the big exception, with ILI remaining very high. NYC has a high rate of the recently evolved XBB strain, which is a possible cause.
https://www.cdc.gov/flu/weekly/index.htm
Matt McIrvin
What makes the situation in the Northeast hard to judge is that we still only have wastewater counts through about December 27th, and while that does cover Christmas, it’s only starting to get into the post-holiday period where the Omicron spike really went vertical last year. It’ll be clearer what we’re dealing with once we have some data extending into the new year.
YY_Sima Qian
@The Moar You Know: Protestations by the Chinese government is pretty cynical & tone deaf. However, the difference is China’s requiring all incoming visitors to test negative on PCR w/in 48 hrs. of departure, masking is still mandated on flights, in the airport on arrival, & all indoor spaces (except restaurants & other eateries) domestically. These new policies by other countries are requiring only arrivals from China to test negative, while testing of inbounds from specific geographical locations has been proven time & again throughout the pandemic to be useless. For the US specifically, the new policy does not come into effect until 1/5, when the infection wave in China is well past peak, when there is no masking mandate in flight or airports, & no further mitigation measures to speak of domestically.
There is also the matter of the XBB.1.5 (1st found in New York), the most worrisome strain currently in circulation, that is spreading fast in the US & from there to the ROW. Meanwhile, it will take a while for new impactful variants to emerge from China (I think Naomi Wu is wrong here). Due to the lack of prior infection, as well as the waning immunity from old vaccines shots that targeted the original Wuhan Variant, there is no evolutionary pressure for the virus to shift toward evading immunity from current strains in circulation. This may change 6 – 12 mo. down the line, after the BF.7/BA.5.2 exit tsunami runs its course in China, & probably a follow on XBB.1.5 wave.
So yes, testing & sequencing arrivals could make sense, & testing & sequencing waste water from inbound flights do make sense, but only if applied to all arrivals. Targeting a single country is performative pretense. COVID-19 is also circulating w/o mitigation in the 80% of humanity outside of China, too. There is no predicting where the next problematic variant might emerge. No one could predict XBB.1.5 would emerge in New York, XBB in SE Asia, BQ.1 in W. Africa, BF.7 in NW Europe, BA.1/2/5 in S. Africa, Delta in S. Asia, Gamma in Brazil, Beta in S. Africa, & Alpha in the UK.
Kim Walker
Does anyone know of a reliable website to track covid in Canada? Provinces are not reporting on covid cases anywhere that I can find, while the media just replays endless variations on health-care systems in crisis. The business community just wants everything to go back to pre-2019, so what we don’t know won’t hurt us (piss us off).
moops
Anecdote:
Abbott lab BinaxNow home test has never given me a positive test result. Yesterday was my 7th day of home quarantine using the FlexFlow home test. BinaxNow says I’m negative. FlexFlow has gone from strong positive, to moderate positive, to very faint but still clearly positive, which has tracked with my symptoms. I’m still symptomatic and I’m very amazed and troubled that Abbott lab’s test is clearing me with a negative test result.
EmbraceYourInnerCrone
@Kim Walker: this is the only information I could find:
COVID-19 epidemiology update
provincial or territorial COVID-19 webpages
smith
@Kim Walker: 91-DIVOC provides data on the provinces, but its data, derived from the Johns Hopkins Center for Systems Science and Engineering (CSSE) data set, I believe ultimately comes from official state, province, or national sources, so if the provinces aren’t reporting, the data there will be incomplete at least.
YY_Sima Qian
@moops: Abbott’s test may not be designed for the current strains.
moops
@YY_Sima Qian:
It shouldn’t matter if we have had mutation and variants
https://covid19.nih.gov/news-and-stories/how-rapid-antigen-tests-perform-against-viral-variants
The current tests should be sensitive across all variants.
but it seems some home tests are not working. Perhaps a batch quality issue? or a batch handling issue? In both those cases the Control line should not appear, but it keeps showing up.
Kim Walker
@smith: Thank you so much!
Kim Walker
@EmbraceYourInnerCrone: Thank you!
frosty
@catclub: I’ve got five vaccinations from five different states. I have my vax record. I think my PCP has it too, if I gave it to her to add to my medical history.
Chetan Murthy
@YY_Sima Qian: YY, I don’t think anybody would imply bad faith on your part. But I do think many of us are surprised at the *incompetence* of the Chinese government. They were doing so well, and then they just squandered all of it. And …. well, despite what you say about how the government couldn’t push the population, many of us are unconvinced that a government that can deploy armies of agents to literally weld doors shut on apartment buildings to enforce quarantine, is literally unable to force people to get vaccinated.
Also, though: when I asked you about this you wrote about Chinese vaccines. But it’s well-understood that Chinese vaccines are pretty weak tea, and we can see that by the way that richer Chinese are traveling to get mRNA shots. The Chinese government could have licensed an mRNA shot, or even simply stolen it. Or license (for free!) Corbevax. Or (hell) just bought Novavax. There were *so* many things that the government could have done, and didn’t, even though it was obvious they needed to.
The incompetence is mind-boggling.
I’ve been reading tweets from Naomi Wu (thanks to Anne’s roundups) for months. I remember her pride and confidence, the way she clapped-back at Westerners who chided her about China’s lockdowns. And now, she’s scared and hurt and outraged because her government has let her down, left her to perhaps suffer and die, and my heart breaks for her and for all Chinese people and residents who must suffer thru this.
Chetan Murthy
@catclub: Heh, y’know, my first thought was: “Huzzah! A chance to get new shots faster!” I’d guess it’s the old state for the old shots and the new state for the new shots. But really, all anybody’s gonna care about, is your most-recent shot.
I got my 5th shot in September, and am looking forward to my next one in February.
PeteS
Paxlovid clearly helped me. I finally got Covid about three weeks ago, despite being 5x vaxxed (which may have saved my life). My GP prescribed Paxlovid after a quick video visit and my symptoms got much less serious within two days, though there were a couple of rocky days after ending the 5-day treatment and occasional wipe-out tiredness for at least another week. Incidentally, I see a specialist regularly, who said there is talk that five days is not enough, it should be 7 or 8, but that is strictly speculative.
Mel
Here’s my take on the “masks don’t work” and the “why bother with mandates” view: masking works if masks are the correct material and are pretty consistently worn correctly by all in high risk public settings.
Masking doesn’t work as well if masks aren’t worn properly or if only high risk individuals are expected to mask, while crowds around them are unmasked. But the more masking in high transmission risk areas, the less transmission, the slower the development of variants, the less illness, the less death.
Masking mandates, flawed and challenging though they may be, do save lives, slow transmission (and thus slow the rapid mutations that lead to storms of immune evasive new variants bombarding us en masse) markedly, and allowseveryone, not just those with obvious risk factors, to have a chance at some semblance of normalcy.
Masking mandates help to protect the obviously vulnerable, but they also protect those with unidentified risk factors. They lessen the chances that healthy, low-risk people will end up battling disabling Long Covid after an infection. They reduce the spread of other respiratory illnesses which can complicate a Covid infection in both healthy and vulnerable people.
But it depends upon most people wearing them correctly and consistently in high risk environments (indoor spaces without adequate ventilation and distancing, public transport, medical facilities, etc.), and thus those mandates need to be consistent and enforced with the support of public health entities and legislation.
Yes, it isn’t easy to overcome the loud noise generated by the most adamant anti-vax, anti-mask crowd. But saving lives now, and lessening the societal, community, and familial impacts of the oncoming massive wave of disability from both initial Covid infections and the growing wave of Long Covid is, in my opinion, worth the effort.
Even if a mandate results in only 85% of people masking correctly in, say, a doctor’s office or a grocery store (ESSENTIAL places where both high-risk and low risk people have to go) it gives tools and reason for telling the remaining 15% to put their mask on or leave, the odds that the other patients, shoppers, etc will be exposed/ infected are reduced.
If all or even the majority of people are masked properly, aerosolization ( you can be infected through cough, sneeze, or speech aerosols that make contact with your eyes as well as through breathing them in) becomes much less of a threat to everyone.
Expecting a mask to protect a single, masked person who is in a room full of aerosol-generating, talking, coughing, sneezing, laughing, unmasked people (some of whom are asymptomatically infected) in the middle of a pandemic is utter nonsense and folly.
It’s not just the aerosols that travel so effectively in the air in enclosed spaces that greatly increase the risk of transmission when there’s no general masking; it is also all the virus that is deposited and stays active / contagious for a period of time on so many commonly shared surfaces. Unmasked, infectious people cough into the air, into their hands, etc. Unmasked people consciously or unconsciously touch their noses, their mouths, their faces much more essily and freely. If ill, every time they rub their nose, wipe their mouth, etc and then touch magazines, doorknobs, pens, clipboards, tabletops, etc., they are spreading Covid, flu, RSV, etc.
So when I hear “if masks really work, then only the vulnerable person needs to wear one, not anybody else”, are nothing but selfishness, misinformation, and honestly, a statement that those with chronic or autoimmune health issues, the immunocompromised, the very young, the elderly, cancer patients, etc. ALL have no human or social value, and can be exterminated without any loss to society as a whole, or at the community or family level.
.”Herd immunity” is obviously about protecting the community and the world at large by ensuring that all who can develop f immunity do, thereby protecting society as a whole, including the vulnerable who cannot develop immunity. Public health policies like vaccine mandates and mask mandates are not just about protecting the public as a whole and as individuals from immediate illness; they are also about protecting individuals and society and from preventable harm that comes from the long term injury and disability incurred by a pandemic or other major health crisis.
I am deeply concerned that so many current policies and practices allow and even encourage preventable mortality and morbidity. Phrases like, “it can’t be helped, it’s just culling the herd”, “it’s their problem, not mine”, “they’re old so they’re likely to die in the next few years anyway…”, “if they’re disabled and they already can’t work anyway, no loss” fly in the face of what sound, ethical public health policy should fight to accomplish. When the head of the CDC shows her unthinking bias by openly stating that it’s “good” that a majority of Covid deaths are vulnerable people (thus, by inference, not the “normal, worthwhile, important, useful” healthy people) we have a public policy problem from the top down.
Say those out things loud, please, if by chance that kind of thinking flits through your mind in a moment of frustration, or if you hear someone saying those things, and please Just really listen to what those statements truly mean. I know that it’s largely preaching to the choir here, posters, lurkers, commenters are deeply good people, but after almost three years of pandemic living, it’s easy to want to wish it away sometimes.
Insert the name of someone you or the other person dearly loves, and then say the statement out loud. “Well, Grandma Esther who raised me and loved me all my life is dead from Covid, but she was old and probably would have died in ten years or so anyway, so it makes no difference that she died now…” “I know that the kids will miss their Dad, but he had asthma, so it’s better that he die so that Covid can cull the herd, so they should stop crying and see it as a long-term plus that he’s not going to be able to weaken the gene pool anymore.” “Hey, Candace, is my best friend, but if she dies from Covid it doesn’t matter, because she isn’t able to work due to her MS. Sorry, but she’s just not contributing to the economy, so she’s no great loss.”
I know, MAGA nuts won’t hear reason. But for someone who is just feeling irritation at being inconvenienced by masking in a visit with their doctor or accountant or for an event, or by a family member asking them to test and mask before visiting, a little reality check about what’s really at stake can shift the conversation, and make it about real people, not politics or temporary inconvenience.
People matter. Here, and out there IRL we matter: the healthy, the vulnerable, the struggling, the stable, the old, the young – none of us should be considered discardable, cull-worthy, worthless because of our age, our status, a glitch in our genes.
Masking correctly and consistently in vital public indoor areas prevents much of the transmission risk from both aerosols and direct touch contamination.
I suspect that most of the people who rant against mask use by saying, “I was forced to wear one at work and still got sick” etc. , refused to wear them properly or consistently, negating the protection they could have had and extended to those around them. My friend who is an NP has named some of them, a little gallows humor: the “chin diaper”, where the mask is covering the chin and part of the lower lip, but nothing that counts; the “no nose for me”, where the mask covers the mouth, but is pulled down so that the entire nose is exposed; the “bottoms up”, where the mask is on, but the wearer pulls it up or down to expose the mouth every time they talk or cough or insist on drinking / eating in a waiting room; the “go team”, where the “mask” is nothing but a flimsy bandana or gaiter, often emblazoned with a logo and intended for fun wear, never as a life saving mask.
This is personal to me, and I apologize if I’ve overstepped or if this is over emotional. I know absolutely that many people don’t need to change their entire lives to make it to the other side of this alive and intact. But there are many people out there who are isolated, struggling to navigate this, and feeling really hopeless about how utterly much of the pandemic response has negated not just their value, but their very existence.
I have lost four people to Covid, and love several more who are struggling every day with Long Covid. I am immunosuppressed. have been forced to isolate for coming up on the third year, with only a short period of glorious relief when vaccine and mask mandates meant that I could pick up groceries and prescriptions, or sit on the porch and talk to my neighbor or my friends, or safely visit the library. And, oh – the relief and the joy of seeing peopke, of being able to do something as simple as safely pick up groceries! Not having to pay for delivery of basic cleaning supplies, medicine, toilet paper (having to pay to be allowed to have access to something essential to life without risking your life to get it – that’s a little more inconvenient than someone having to wear a mask for 40 minutes while in a grocery store, no?).
Every time I see the delivery and service fees, I wince, but I also wonder – what would I have had to do to survive if I were at the point I was at 10 years ago, when we had spent every penny of our savings and retirement to pay medical bills and were just barely keeping a roof over our heads day to day? What is happening right now to people in the same position, for whom those 10, 20, or 30 dollars a week mean the difference between eating or not eating, being safe or risking your life to pick up your life-saving prescription?
I have not been able to hug or read to or snuggle my precious little nieces or nephews for three years. They are more than happy to mask, but with constant school exposure to unmasked classmates, it becomes pointless for them to try. So, we miss each other terribly, and I am not able to be there with them for all the little moments that matter.
Now, with mask mandates gone and immune evasive variants emerging, it is truly risky for me to even go to a medical appointment, as all but one of my doctors’ medical groups no longer require any masking.. One doctor’s group allows people with respiratory illness to sit in the waiting areas with everyone else, as long as they answer “no” to “have you been in contact with someone who has Covid?” and “have you travelled outside the country in the past 10 days” questions. My doctor is horrified, but powerless to change the policy, since the CDC decreed that masking is entirely optional and a matter of choice even in med facilities.
My sibling, a lifelong teacher who was a coach and avid cyclist, hiker, camper, runner now struggles daily with Long Covid.
My friend’s healthy, active, 31 year old son (who is also a new Dad), had sudden heart failure while at work, was in a coma for a couple of weeks, and sustained ensuing brain damage due to the heart failure and resulting lack of oxygen before he was resuscitated, all from a largely asymptomatic case of Covid. He “felt a little tired” but chalked that up to the late nights with the new baby. He is now disabled for life. His family’s entire lives changed in the blink of an eye. If his place of work had had vaccine and mask mandates in place, if the public health messaging had communicated that even the apparently healthy can sometimes experience serious Covid consequences and should take basic precautions for their own protection as well as for others’ protection, it’s more likely that their tragedy and many others like it could be avoided.
I’m not asking to argue or debate any of the above. I know that everyone just wants a simple, functional, normal life, and damn, how hard this pandemic has been on everyone, in so many different ways. I’m just hopeful that sharing this clarifies a bit of what it’s like to be living with this pandemic as somehow who is high-risk, and why I am so convinced that without any further organized, effective public health interventions, like masking, we have slim chance of controlling the rapid development of immune evasive variants and less chance of preventing the snowballing long-term consequences of this pandemic.
YY_Sima Qian
@Chetan Murthy: Dead thread, but…
I have tried too address these points in my comments to A.L.’s regular COVID-19 posts. In a couple of weeks, as the exit tsunami in China subsides, & we have a better hindsight into what has happened in China, I may do another guest post to organize my thoughts & address the issues more comprehensively.
Overall the analytical framework I believe in is assessing what the CCP regime realistically could have & should have done prior to opening, & that should be the focus of criticism. We should also be realistic about the potential impact of the actions that could have & should have been taken. We can also assess what would have been inevitable, even if the CCP regime prepared as well as the best performing countries in managing the pandemic, for that we can reference the experiences of other former Zero COVID countries/regions as they opened while accounting for differences in demographics & health care resources.