My company is in the middle of the 2015 product development cycle. The actuaries are getting a viable clue, the medical management folks are starting to see populations that are large enough to draw reasonable inferences, and our finance folks are seeing the money come in and out. The project managers are cooridinating and deconflicting …
PPO, EPO and HMO — what is the difference?Post + Comments (17)
The biggest difference between these three types of plan organization is the amount of control and choice available. HMO’s tend to be the most restrictive while PPO’s tend to offer the most flexibility. All else being equal, HMO’s tend to be significantly less expensive than an equivilent PPO because choice is costly as the HMO is a medical utilization control system while the PPO has always been about minimal hassle access to anything.
The Massachusett’s state employee web page has a good explainer:
If you are in an HMO, you must use network providers… An HMO requires the selection of a Primary Care Physician (PCP) to manage your care. Referrals are usually needed…
with an EPO you must use network providers… Unlike an HMO, you do not need to select a Primary Care Physician, nor do you need to contact your PCP for referrals to specialists…
With a PPO, you receive more comprehensive benefits by using network providers… You have the option of using non-network providers… With a PPO, you do not need to select a Primary Care Physician.
Network size is fundamentally irrelevant. An HMO can have 100,000 providers in it while a PPO can have only 3,000 providers in that network. The difference is the control and choice restriction.
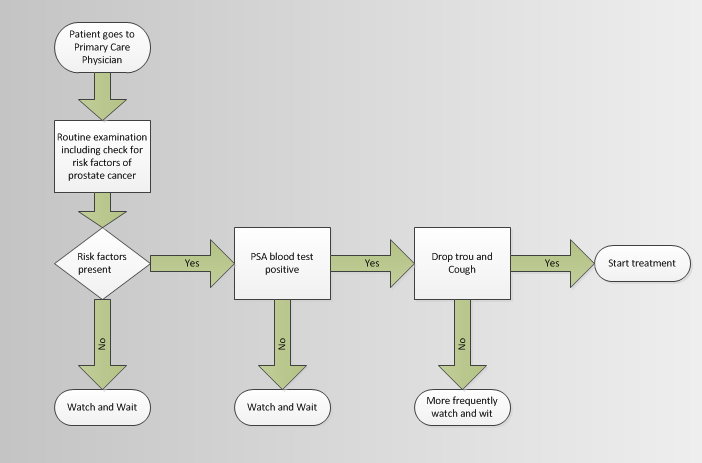
HMO’s are the most restrictive and they tend to have different payment models than PPOs. HMO’s since they restrict choice are able to tie patients to particular providers. Patients are supposed to go through their primary care physicians (PCP) for all care. A patient who jacks up their ankle should see their PCP first. If the ankle is truly jacked up, the PCP will write a referral for an orthopedist and PT. If the ankle is only slightly jacked-up, rest, ice, compression and elevation would be the course of action.
The PCP is supposed to coordinate care between the PCP, specialist, and any ancillary/hospital services a patient needs. Some HMOs will pay the PCP a fixed fee per patient per month and all other costs come out of that fee. This theoretically aligns the treatment incentives so that patients only get the care they need at reasonably prices.
EPOs are have softer control mechanism. Patients are not required to have a dedicated PCP. Patients direct their own care with the advice of their PCP. EPOs are popular because they tend to have lower costs than PPOs but have fewer restrictions than HMOs. Under an EPO set-up, a patient who jacks up their ankle can go to straight to an in-network orthopedist instead of going to their primary care physician.
PPOs have minimal control over patient choices. Patients can go anywhere. In network providers get a better deductible and co-insurance rates. The same person with a jacked-up ankle can go see an in-network orthopedist at low co-pay and low deductible. However, if a patient wants to go see an orthopedist two time zones away who regularly fixes running backs, the insurance company will pay some of usual and customary charges of the out of network provider.
PPOs often a significant amount of flexibility. But since they fundamentally don’t say no to any care choice, they tend to be much more expensive.