
The Duke Margolis Center for Health Policy and several co-authors from other institutions in work funded by the Rockefeller Foundation has issued a new analysis on how we can use testing to reduce community transmission and thus more safely operate key infrastructure, facilities and services.
One of the big-takeaways from this report that I got as I was writing was the wide variety of approaches that are capable of achieving a variety of goals. There are a lot of different testing technologies out there. We really care about two primary characteristics of a test; how sensitive is it and how quickly can a result be reported back? The ideal test is a perfectly sensitive test that will only report true positives (100% sensitive) in two seconds or less and costs less than a pack of supermarket check-out line gum. That test does not exist. Everything is a trade-off and the trade-off space is quite large and varied. I love Figure 2 as it illustrates what communities could potentially do:
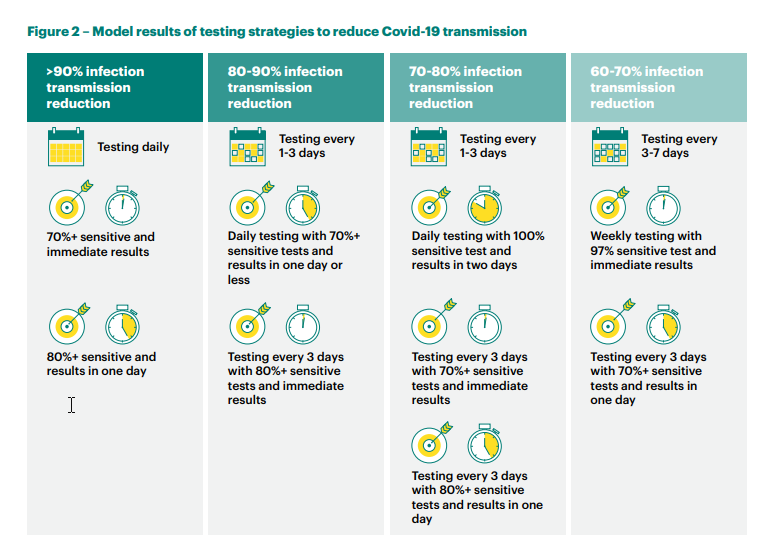
A community can choose a targeted reduction in the current (R)eproductive rate and then apply a variety of tests. Given that national R is around 1 which means each infected person will infect on average about 1 other person and therefore the daily new case count is roughly stable, a 60% reduction and a 90% reduction in R both mean that the epidemic burns itself out fairly quickly. The quick rule of thumb is that more sensitive tests with slightly slower turn-around times are roughly equal to less sensitive tests with fast results.
The National Football League has taken a choice of very sensitive PCR tests conducted on a daily cadence with results reported within 24 hours to wipe out within-team transmission:
It has worked!
Latest COVID numbers, via the NFL: From Aug. 30-Sep. 5, the league conducted 17,519 COVID-19 tests to players. Only one player tested positive.
— NFL Update (@MySportsUpdate) September 8, 2020
This is overkill and rubble bouncing from a public health perspective. The goal is to significantly reduce local R in order to make clusters become singletons and avoid large infection chains. Once community prevalence is down, good things can and should happen like kids going back to school. We can do that soon. We don’t quite have the current cheap enough and good enough testing supply but within the next few months, hundreds of millions of cheap enough, good enough and fast enough tests will be hitting the US market. That will allow us to test our way out of trouble.
Lots of ways to suppress community spreadPost + Comments (28)