President Trump has stated that he wants a new healthcare proposal. His budget called from major Medicaid and exchange cuts as well as the Graham-Cassidy framework of state blockgrants to cover far fewer people in the exchange and Medicaid expansion populations.
It's been like 3 weeks since the Graham-Cassidy approach to ACA repeal was proposed in the President's Budget, which most definitely did not protect coverage for people w/ pre-existing conditions currently benefiting from the ACA's protections.https://t.co/li1dbkKyAT https://t.co/laUrMHAm4E
— Loren Adler (@LorenAdler) April 1, 2019
In the short run this is irrelevant. There probably are fifty one votes in the Senate for something like Graham-Cassidy to pass. The Majority Leader would be willing to schedule that vote.
There are not 218 votes in the House to pass Graham-Cassidy. Nor is there a Speaker willing to schedule a vote on Graham-Cassidy if it was likely to pass.
However, it is worthwhile to look at the logic of the plan. It is a major cut to federal spending and a major redistribution of federal spending. Right now, more federal money goes to states that aggressively implement the Affordable Care Act or have very high cost markets. That means states like California which aggressively outreach for every single possible enrollment and expanded Medicaid will get more federal ACA money than states like Mississippi or South Dakota which have not expanded Medicaid and have not aggressively pushed enrollment on the Exchanges.
Graham-Cassidy wants to give block grants to states that over time converge to a narrow band on a per-capita basis. It reduces the overall pool of money available and then shifts the remaining funds to states that have done opposed the ACA’s implementation. There were variants where money would be freed up to throw at Senators from states that had implemented the ACA and Medicaid Expansion aggressively but whose votes might be needed to pass the bill.
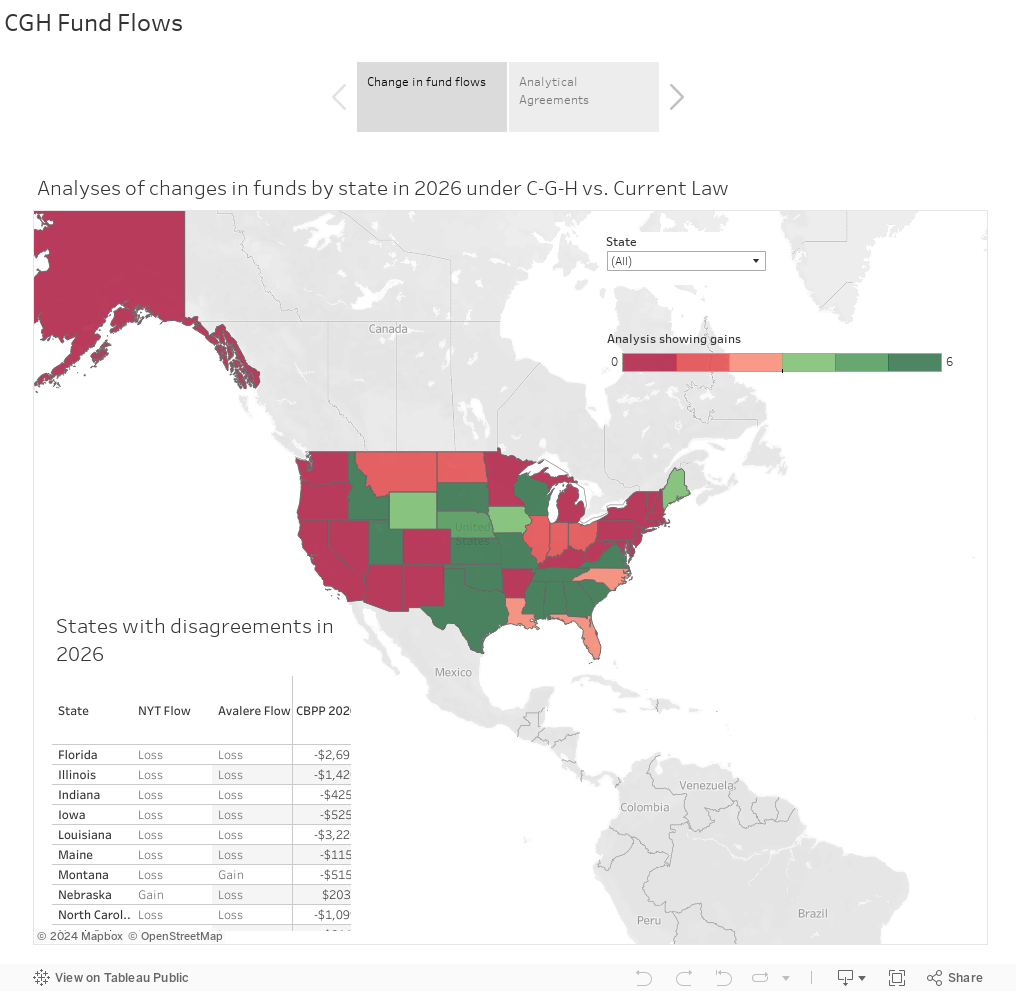
During the summer of 2017, I tracked the outside evaluation of federal fund flows to states in 2026 under the counter-factual of Graham-Cassidy being implemented and current law of the ACA with CSR funding as the baseline. The coastal states got hammered while the Great Plains, Mountain West and the Deep Confederacy did well.
Circumstances have changed. The three major changes are more states have expanded Medicaid since September 2017, the termination of CSR payments increased effective net subsidies for more people and the elimination of the individual mandate probably depressed enrollment. The 2017 scores will need to be updated, but I think a 2019 score of Graham-Cassidy would be similar.